Eating Behaviour Revision Notes
Subject: Psychology | Level: A-Level | Exam Board: AQA
This guide provides a comprehensive analysis of Eating Behaviour for AQA A-Level Psychology, focusing on the critical interplay between biological and psychological explanations. It is designed to equip candidates with the precise knowledge and evaluative skills required to deconstruct 16-mark questions and achieve top-band marks in Paper 3.
Revision Notes & Key Concepts
Key Terms & Definitions
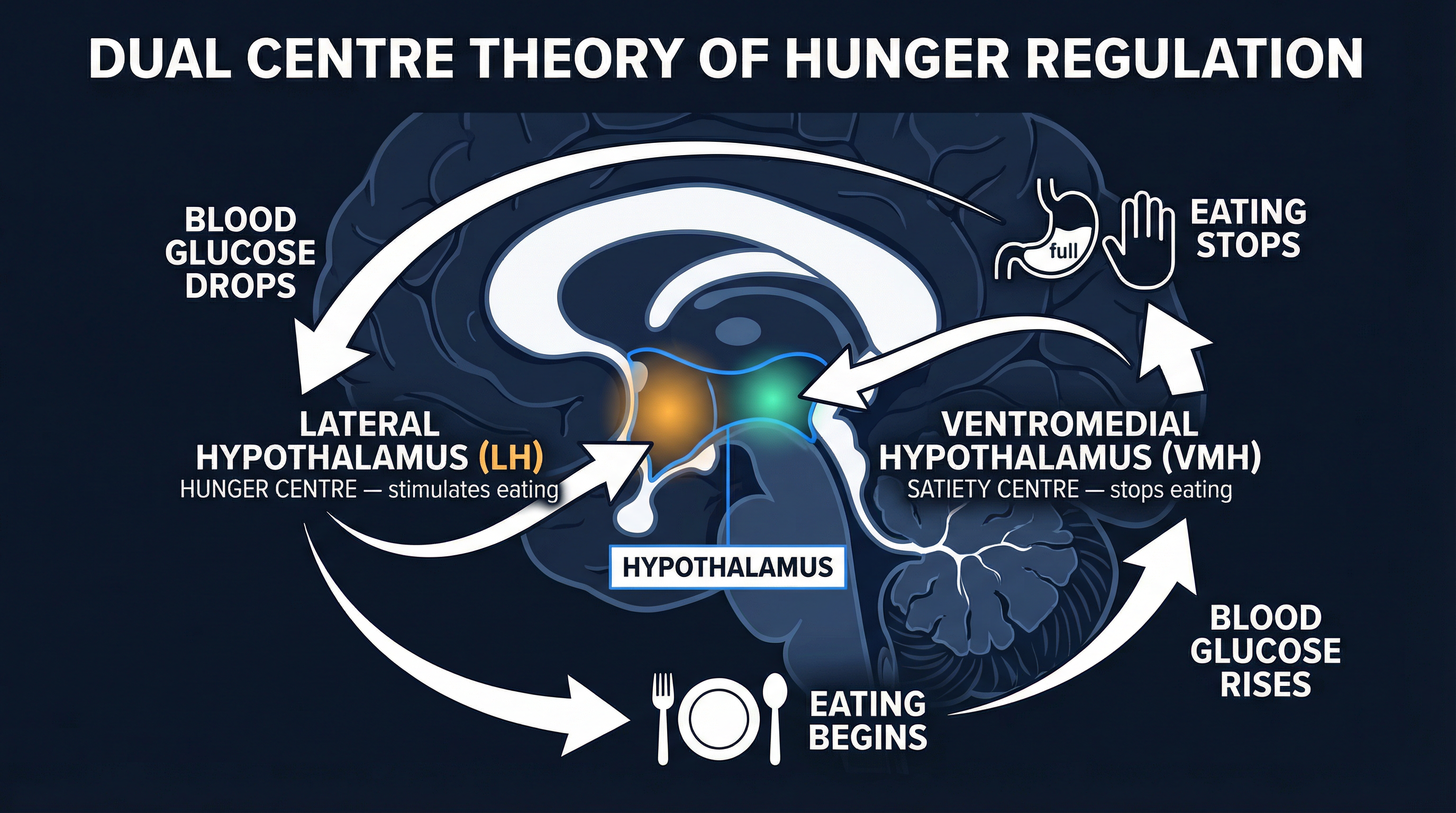
- Lateral Hypothalamus (LH)
- A part of the hypothalamus identified as the 'feeding centre', responsible for initiating eating behaviour.
- Ventromedial Hypothalamus (VMH)
- A part of the hypothalamus identified as the 'satiety centre', responsible for stopping eating behaviour.
- Neophobia
- An innate fear or reluctance to try new foods.
- Enmeshment
- A characteristic of dysfunctional families where boundaries are unclear and members are overly involved in each other's lives.
- Restrained Eater
- An individual who consciously limits their food intake to control their body weight (a dieter).
- Disinhibition
- The breakdown of self-imposed cognitive control, leading to impulsive behaviour. In dieting, this is the 'what-the-hell' effect.
Worked Examples
Worked Example
Question: Discuss evolutionary explanations for food preferences. (16 marks)
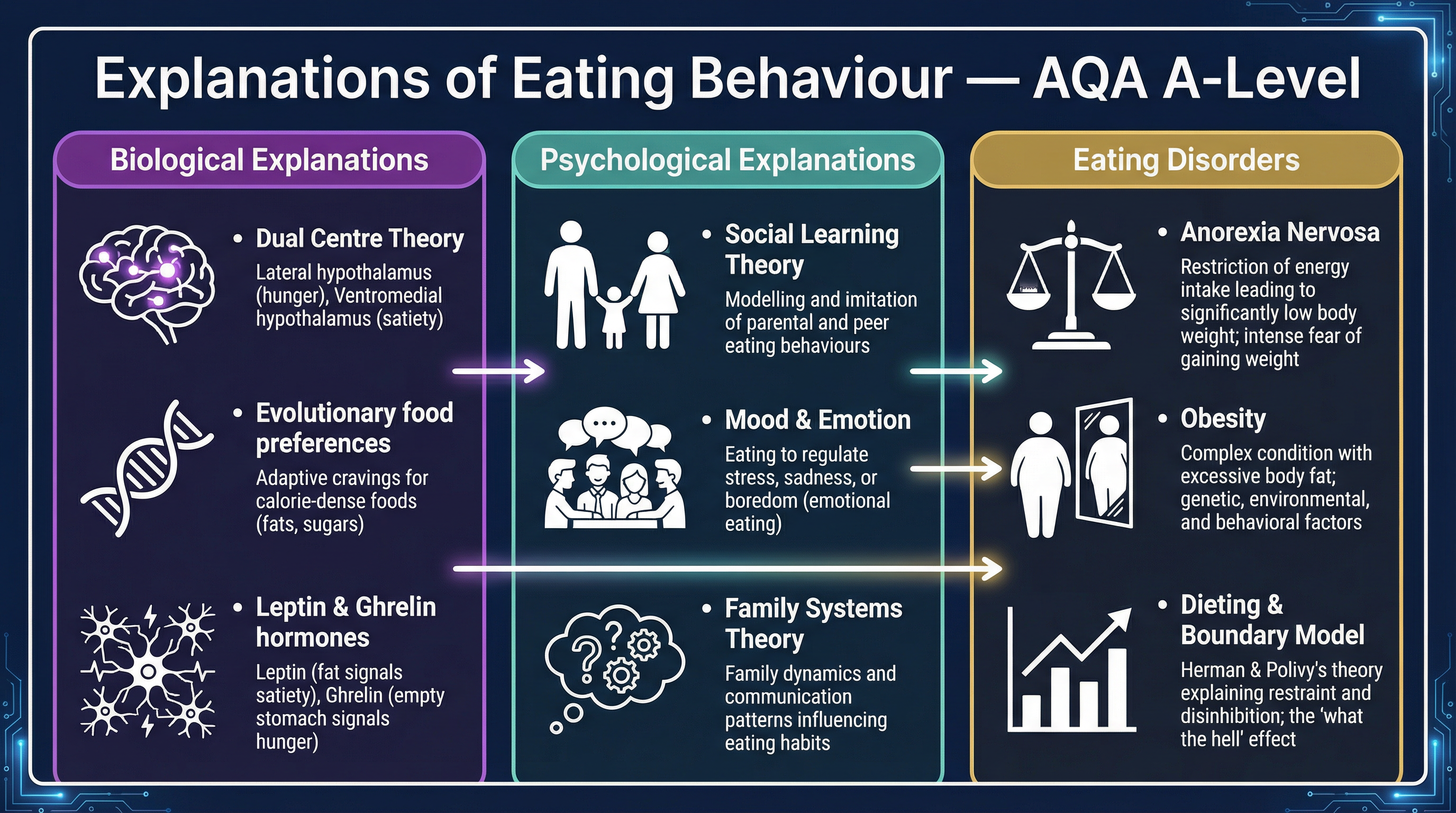
Solution: **Introduction**: Evolutionary explanations propose that our modern food preferences are adaptations inherited from our ancestors in the Environment of Evolutionary Adaptedness (EEA). These preferences, such as for sweet and fatty foods, were adaptive because they provided crucial calories in an environment of scarcity, thus enhancing survival and reproduction. This essay will outline these explanations before evaluating them in terms of supporting evidence and competing theories. **Paragraph 1 - AO1: Preference for Sweetness and Fat**: An innate preference for sweetness is evident from birth, as it signals a safe source of high-energy carbohydrates. For example, Steiner (1977) found that newborns showed positive facial expressions when tasting sweet substances. Similarly, a preference for fatty foods would have been highly adaptive, as fat is the most calorie-dense energy source available. In the EEA, these preferences would have driven our ancestors to seek out rare but vital resources like ripe fruit and animal fats, increasing their chances of survival. **Paragraph 2 - AO1: Neophobia and Taste Aversion**: Evolutionary pressures also shaped our avoidances. Neophobia, an innate reluctance to try new foods, is adaptive for young children as it reduces the risk of them ingesting toxic substances. Birch (1999) suggests it appears around the time children begin to explore independently. Taste aversion is a form of biological preparedness where we quickly learn to associate the taste of a food with illness. If an ancestor became sick after eating a new plant, they would avoid it in the future, a life-saving adaptation. **Paragraph 3 - AO3: Strength - Supporting Research**: There is research support for the role of evolution in food preferences. For instance, the universality of certain facial expressions in response to tastes (e.g., sweet, sour, bitter) across different cultures suggests an innate, biological basis rather than a learned one. This strengthens the claim that these preferences are a product of evolution. **Paragraph 4 - AO3: Weakness - Reductionism**: The evolutionary explanation is biologically reductionist. It reduces the complexity of food choice to innate genetic pressures, largely ignoring the significant and well-documented influence of learning and culture. For example, Social Learning Theory provides a compelling explanation for how children acquire the food preferences of their parents and peers, which cannot be accounted for by evolution alone. The sheer diversity of cultural diets demonstrates that learning plays a crucial role. **Paragraph 5 - AO3: Weakness - Competing Explanations**: Furthermore, the evolutionary explanation struggles to account for individual differences. For example, it cannot easily explain disorders like anorexia nervosa, where individuals deliberately starve themselves, directly contradicting the evolutionary drive to consume calories. Psychological explanations, such as Family Systems Theory or cognitive theories focusing on control and perfectionism, provide a more plausible account for such maladaptive eating behaviours. **Conclusion**: In conclusion, while evolutionary explanations provide a powerful and logical account for the origins of certain innate food preferences, they offer an incomplete picture. They are reductionist and fail to account for the significant impact of social learning, culture, and individual cognition. A more comprehensive understanding requires an interactionist approach, acknowledging that while we may have innate predispositions, these are heavily shaped and modified by our environment and experiences.
Worked Example
Question: Outline and evaluate one psychological explanation for anorexia nervosa. (16 marks)
Solution: **Introduction**: Family Systems Theory (FST), proposed by Minuchin et al. (1978), is a key psychological explanation for anorexia nervosa (AN). It posits that AN is not an individual pathology but a symptom of a dysfunctional family system. This essay will outline the key features of the 'psychosomatic family' before evaluating the theory using supporting evidence and considering alternative explanations. **Paragraph 1 - AO1: Enmeshment and Overprotectiveness**: FST identifies several key features of families where a member develops AN. Enmeshment refers to a lack of boundaries, where family members are overly involved in each other's lives, stifling any sense of individuality. This is often coupled with overprotectiveness, where the family constantly protects its members from external threats, reinforcing their interdependence and making it difficult for the adolescent to develop autonomy. **Paragraph 2 - AO1: Rigidity and Conflict Avoidance**: Rigidity is the tendency for the family to resist change and maintain the status quo. When faced with a crisis, the family is too inflexible to adapt its structure or rules. Conflict avoidance is the suppression of open disagreement. Problems are left to simmer, rather than being resolved. Within this context, the adolescent's refusal to eat can be seen as a desperate, non-verbal attempt to assert control and independence in a system that denies them a voice. **Paragraph 3 - AO3: Strength - Supporting Evidence**: There is research to support the link between these family characteristics and AN. Strauss and Ryan (1987) found that female anorexics demonstrated greater disturbances in autonomy and a more controlling family style compared to a control group. Furthermore, Minuchin et al. (1978) reported an 86% success rate from using Family Therapy to treat AN, which involves restructuring family dynamics. This therapeutic success provides strong pragmatic support for the theory's core assumptions. **Paragraph 4 - AO3: Weakness - Cause and Effect**: A significant limitation of FST is the problem of establishing cause and effect. It is unclear whether the dysfunctional family patterns cause anorexia, or whether the stress of living with an anorexic child causes the family dynamics to become enmeshed and rigid. It is plausible that the family's behaviour is a reaction to the illness, not its cause. This correlational evidence makes it difficult to draw firm conclusions about the theory's validity. **Paragraph 5 - AO3: Weakness - Incomplete Explanation**: FST provides an incomplete explanation as it largely ignores biological factors. There is strong evidence for a genetic component to AN, as shown by Holland et al.'s (1988) twin study which found a 56% concordance rate in MZ twins. A diathesis-stress model may be more appropriate, suggesting that individuals may have a genetic vulnerability (diathesis) which is then triggered by the family and wider cultural stressors that FST describes. This interactionist perspective offers a more holistic and plausible account. **Conclusion**: In conclusion, Family Systems Theory provides a valuable insight into the role of family dynamics in the development of anorexia nervosa, and its therapeutic applications have shown considerable success. However, its failure to establish causality and its neglect of biological factors are significant limitations. The theory is best seen as one part of a wider, interactionist explanation for this complex disorder.
Worked Example
Question: Outline and evaluate the Boundary Model of dieting. (8 marks)
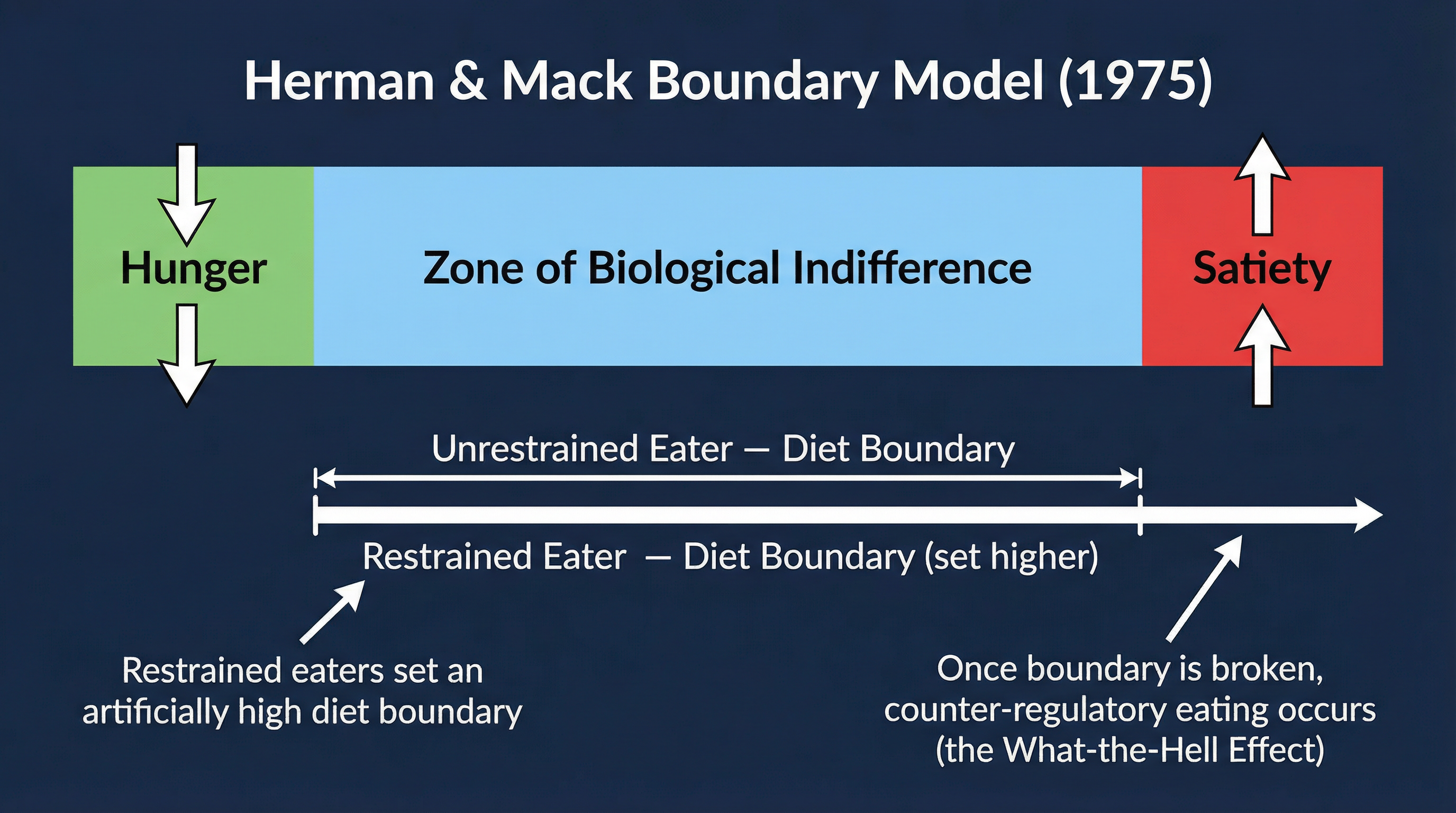
Solution: **Outline (AO1)**: The Boundary Model, proposed by Herman and Mack (1975), explains the failure of dieting. It suggests that our eating is regulated by a physiological hunger boundary and a satiety boundary. Between these lies the 'zone of biological indifference'. Restrained eaters (dieters) impose an additional cognitive 'diet boundary' within this zone. The model predicts that if this cognitive boundary is crossed, dieters experience the 'what-the-hell' effect, abandoning all restraint and overeating (disinhibition), often consuming more than a non-dieter. **Evaluation (AO3)**: A strength of the model is the supporting evidence from Wardle and Beales (1988). They found that women in a diet group ate more in a subsequent taste test than women in an exercise or control group, supporting the concept of counter-regulatory eating. However, a limitation is that the model is a cognitive explanation that largely ignores biological factors. For example, it doesn't account for the role of hormones like leptin and ghrelin in appetite regulation. Therefore, it could be seen as reductionist, as it oversimplifies the complex interaction of biological and psychological factors in dieting behaviour.
Practice Questions
Question: Outline the role of ghrelin and leptin in the control of eating behaviour. (4 marks)
Answer:
Question: Describe and evaluate one study of social learning and food preferences. (8 marks)
Answer:
Question: A psychologist was interested in the link between mood and eating. She asked 20 participants to watch a sad film and 20 different participants to watch a neutral film. All participants were given a large bowl of popcorn. The psychologist measured how many grams of popcorn each participant ate. She found that the participants who watched the sad film ate significantly more popcorn than those who watched the neutral film. Explain how this study could be improved by using a repeated measures design. (4 marks)
Answer:
Question: Discuss biological explanations for anorexia nervosa. (16 marks)
Answer:
Question: Outline what is meant by 'disinhibition' in the context of dieting. (3 marks)
Answer: