Schizophrenia Revision Notes
Subject: Psychology | Level: A-Level | Exam Board: AQA
Schizophrenia is a complex and severe mental disorder that represents a cornerstone of AQA A-Level Psychology Paper 3. This guide deconstructs the essential knowledge, from classification and symptoms to biological and psychological explanations, providing the critical evaluation skills needed to achieve top marks.
Revision Notes & Key Concepts
Revision Podcast Transcript
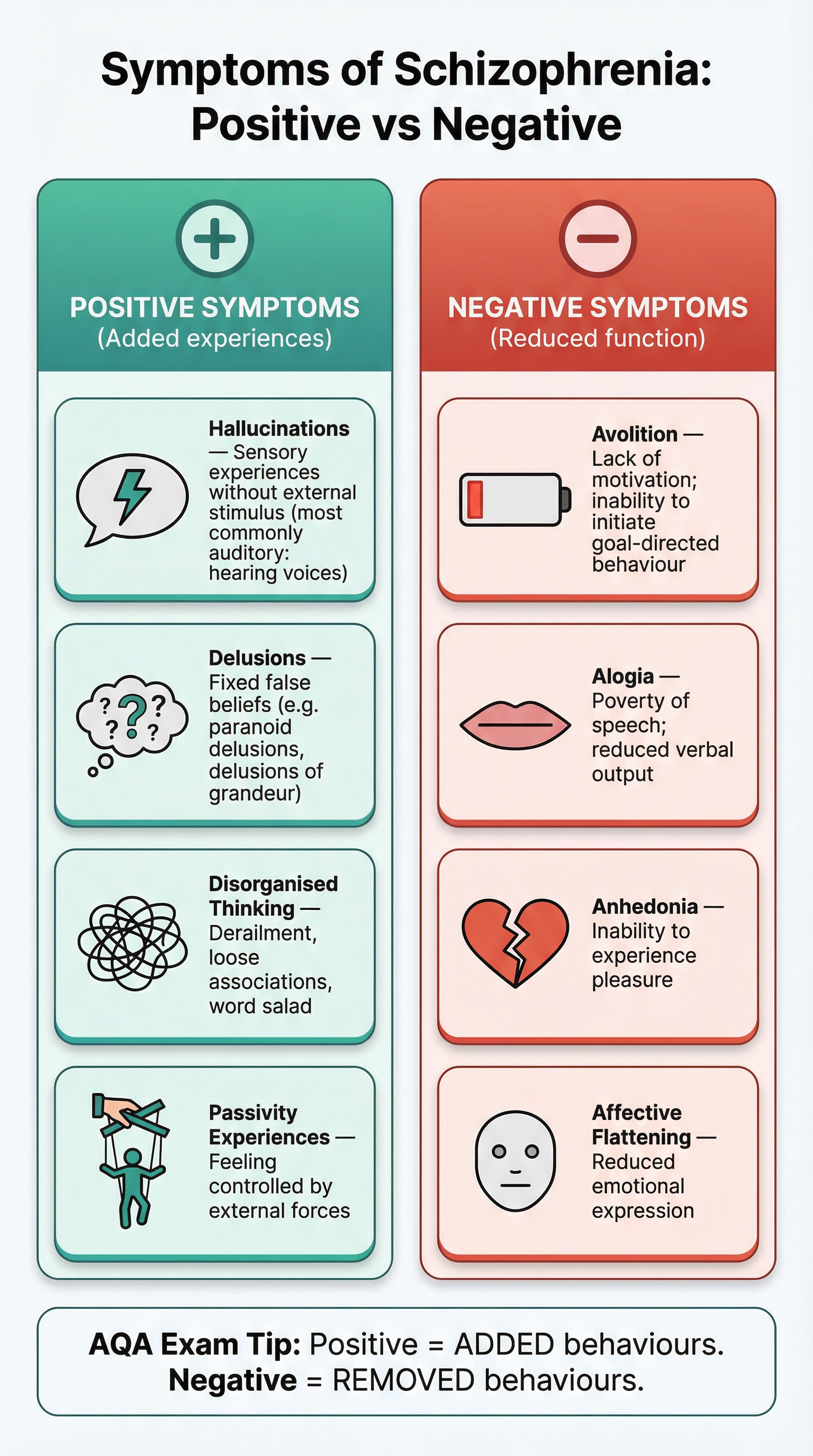
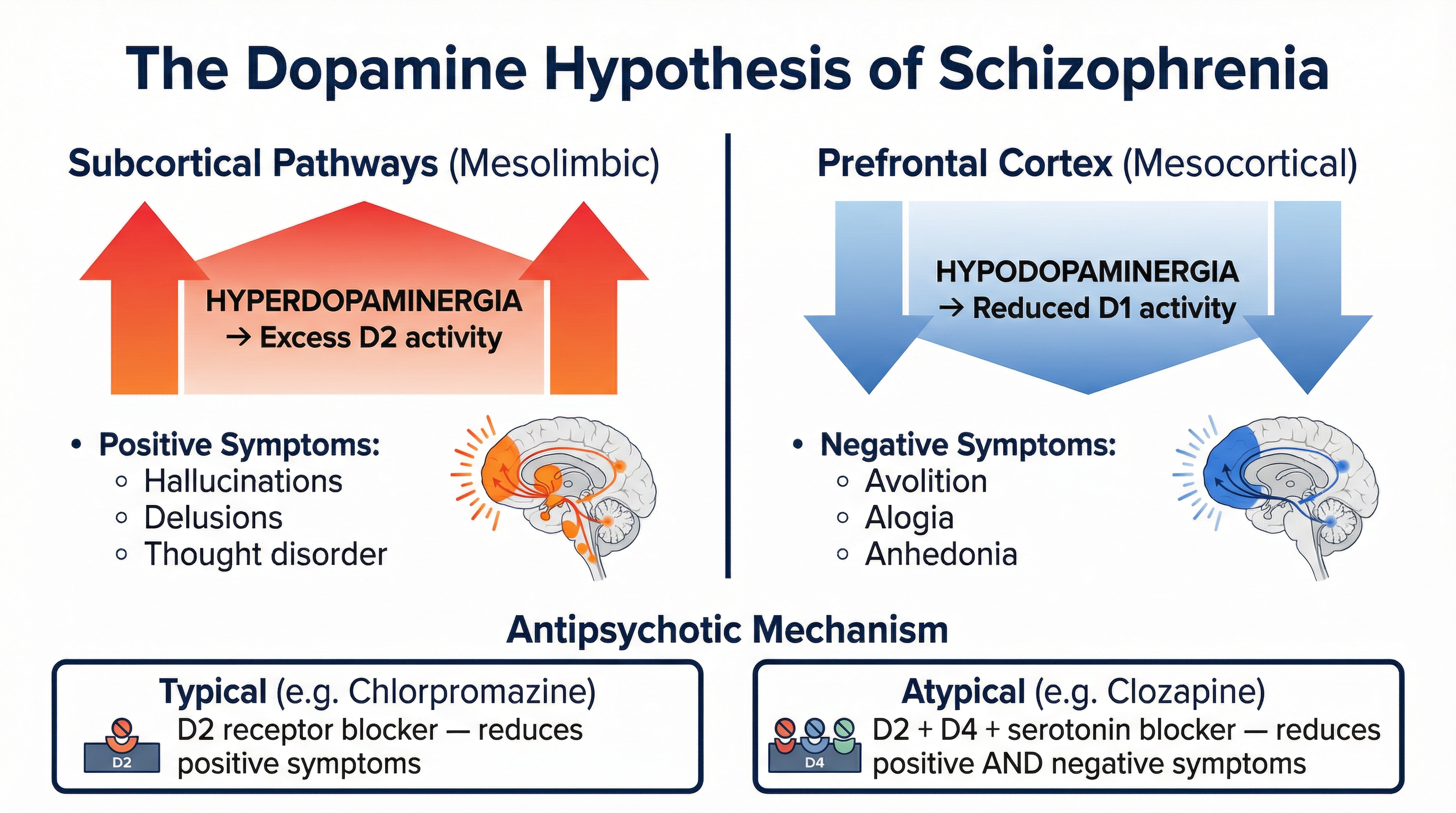
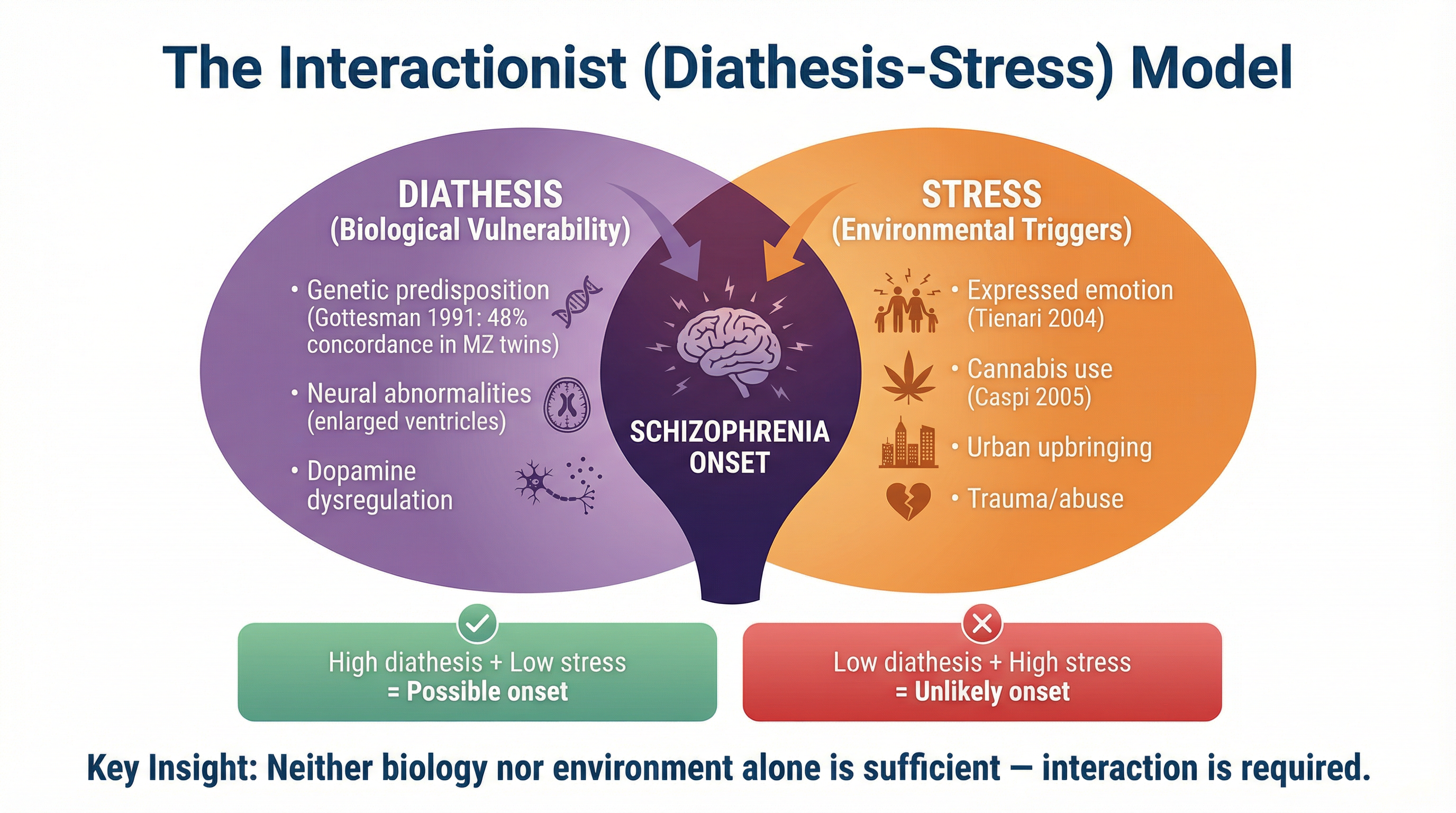
Welcome to your AQA A-Level Psychology revision podcast. I'm your tutor for today, and we're diving deep into one of the most fascinating and exam-rich topics on Paper 3: Schizophrenia. Whether you're revising for the first time or doing a final polish before your exam, this episode is going to give you everything you need — the core content, the evaluation points examiners love, and the common mistakes that cost students marks every single year. So let's get into it. Schizophrenia is a severe mental disorder affecting approximately one percent of the population worldwide. It's characterised by a profound disruption in thinking, perception, and emotional regulation. For your AQA exam, this topic sits on Paper 3, and it's one of the highest-value topics you can revise — questions can be worth up to 16 marks. The examiners want to see that you understand not just what schizophrenia is, but how it's classified, what causes it, and how it's treated — and crucially, that you can evaluate all of these things with real evidence. Let's start with classification and diagnosis. The two main classification systems you need to know are the DSM-5 — that's the Diagnostic and Statistical Manual, fifth edition, published by the American Psychiatric Association — and the ICD-10, the International Classification of Diseases, tenth edition, published by the World Health Organisation. Both systems require the presence of symptoms for a minimum duration, but they differ in important ways. The DSM-5 requires at least two of five key symptoms — delusions, hallucinations, disorganised speech, disorganised behaviour, and negative symptoms — to be present for at least six months. The ICD-10 has a lower threshold and places more emphasis on first-rank symptoms, which were originally described by Kurt Schneider. Now, symptoms. This is absolutely fundamental, and examiners will credit you for making a precise distinction between positive and negative symptoms. Positive symptoms are those that are added to normal experience — they represent an excess or distortion of normal function. The key positive symptoms are hallucinations, which are sensory experiences without an external stimulus — most commonly auditory hallucinations, where the patient hears voices. Then there are delusions, which are fixed false beliefs that are not amenable to reason — for example, paranoid delusions where the patient believes they are being persecuted, or delusions of grandeur where they believe they have special powers. Disorganised thinking, sometimes called formal thought disorder, is also a positive symptom — this includes derailment, where the patient jumps between unrelated topics, and in severe cases, word salad, where speech becomes completely incoherent. Finally, passivity experiences — feeling that one's thoughts or actions are being controlled by an external force. Negative symptoms, by contrast, represent a reduction or loss of normal function. Think of them as what gets taken away. The key ones are avolition — a profound lack of motivation and inability to initiate goal-directed behaviour. Alogia — poverty of speech, where the patient produces very little verbal output. Anhedonia — the inability to experience pleasure. And affective flattening — a reduction in the range and intensity of emotional expression. Here's a memory hook for you: Positive symptoms are ADDED — think of a plus sign. Negative symptoms are REMOVED — think of a minus sign. Simple, but it works. Now let's talk about the biological explanations. The dopamine hypothesis is the cornerstone of the biological approach to schizophrenia, and you need to know it in detail. The original dopamine hypothesis proposed that schizophrenia is caused by an excess of dopamine activity — specifically, overactivity at D2 receptors. This was supported by two key pieces of evidence: first, antipsychotic drugs that block D2 receptors reduce positive symptoms; second, drugs that increase dopamine activity, like amphetamines, can induce psychotic symptoms in healthy individuals. However, the revised dopamine hypothesis is more sophisticated and more accurate — and this is what examiners want to see. The revised hypothesis distinguishes between two dopamine pathways. In the mesolimbic pathway, which connects the ventral tegmental area to the limbic system and the ventral striatum, there is hyperdopaminergia — that means too much dopamine activity. This excess activity at D2 receptors in the subcortex is linked to positive symptoms like hallucinations and delusions. In the mesocortical pathway, which connects to the prefrontal cortex, there is hypodopaminergia — too little dopamine activity. This reduced activity at D1 receptors in the prefrontal cortex is linked to negative symptoms like avolition and alogia. This is a really important distinction. Examiners will specifically credit candidates who link the ventral striatum hyperdopaminergia to positive symptoms, and prefrontal cortex hypodopaminergia to negative symptoms. Don't just say "too much dopamine" — be specific about the pathway and the symptom type. Now, the genetic explanation. There is strong evidence for a genetic component to schizophrenia. The key study here is Gottesman's 1991 review of twin and family studies. Gottesman found that the concordance rate for schizophrenia in monozygotic — that's identical — twins is approximately 48 percent. For dizygotic — fraternal — twins, it drops to around 17 percent. For first-degree relatives, it's around 9 percent, and for the general population, it's about 1 percent. This pattern strongly suggests a genetic component. However — and this is crucial for evaluation — the concordance rate in identical twins is only 48 percent, not 100 percent. If schizophrenia were purely genetic, identical twins should have a 100 percent concordance rate. This tells us that genes alone cannot explain schizophrenia, and that environmental factors must also play a role. Neural correlates are another biological explanation. Research using brain scanning technology has identified structural abnormalities in the brains of people with schizophrenia. Enlarged ventricles — the fluid-filled spaces in the brain — have been found in many patients. This suggests a loss of brain tissue. Studies have also found reduced grey matter volume in the prefrontal cortex and temporal lobes. However, it's important to note that these neural differences could be a consequence of schizophrenia rather than a cause — or they could be caused by antipsychotic medication rather than the disorder itself. This is a key evaluation point. Now let's move to psychological explanations. The cognitive explanation focuses on faulty information processing. Frith proposed that people with schizophrenia have a deficit in metarepresentation — the ability to reflect on one's own thoughts and intentions. This could explain why patients experience their own thoughts as external voices — they cannot recognise their own internal mental states as belonging to themselves. Frith also proposed a deficit in central control — the inability to suppress automatic responses to stimuli — which could explain disorganised thinking and speech. The family dysfunction explanation includes two theories you need to handle carefully. The schizophrenogenic mother theory, proposed by Fromm-Reichmann in 1948, suggested that cold, rejecting, and overprotective mothers created an environment that caused schizophrenia in their children. The double bind theory, proposed by Bateson and colleagues in 1956, suggested that children who receive contradictory messages from parents — for example, being told verbally that they are loved while being shown physical rejection — develop confused thinking patterns that lead to schizophrenia. Now, here's the critical point: you must acknowledge that these theories have very little empirical support and are considered socially sensitive. They have been largely discredited and can cause significant harm by placing blame on families. Examiners will not credit uncritical presentation of these theories. The expressed emotion model, however, is more empirically supported. Expressed emotion refers to the level of criticism, hostility, and emotional over-involvement expressed by family members towards a patient. High expressed emotion environments are associated with higher relapse rates. Tienari's 2004 Finnish Adoptive Family Study found that adopted children of biological mothers with schizophrenia were more likely to develop the disorder if they were raised in high expressed emotion family environments — but not if they were raised in healthy family environments. This is powerful evidence for the interaction between genetic vulnerability and environmental stress. Now for therapies. There are two main biological therapies: typical antipsychotics and atypical antipsychotics. Typical antipsychotics, like Chlorpromazine, work primarily by blocking D2 dopamine receptors in the mesolimbic pathway. This reduces positive symptoms — hallucinations and delusions — but has little effect on negative symptoms. In fact, by blocking dopamine in the mesocortical pathway, typical antipsychotics can actually worsen negative symptoms. They also carry significant side effects, including tardive dyskinesia — involuntary repetitive movements — and extrapyramidal side effects like Parkinsonism. Atypical antipsychotics, like Clozapine and Risperidone, have a broader mechanism of action. Clozapine blocks D2, D4, and serotonin receptors. This means it can reduce both positive and negative symptoms. Clozapine is considered the most effective antipsychotic available, but it carries a serious risk of agranulocytosis — a potentially fatal reduction in white blood cells — which means patients must have regular blood tests. This is a key evaluation point: the effectiveness of Clozapine must be weighed against its serious side effects and the ethical implications of requiring ongoing medical monitoring. The key psychological therapy is Cognitive Behavioural Therapy for Psychosis, or CBTp. CBTp aims to help patients identify and challenge the distorted thinking patterns that underlie their symptoms. For example, a patient who believes they are being persecuted might be helped to consider alternative explanations for the experiences they are having. CBTp does not aim to eliminate symptoms entirely, but to reduce the distress they cause and improve functioning. The NICE guidelines recommend CBTp as a first-line treatment for schizophrenia, to be used alongside medication. Meta-analyses, including work by Wykes and colleagues in 2008, have found moderate effect sizes for CBTp in reducing positive symptoms. Family therapy is also on the specification. It aims to reduce expressed emotion in the family environment, thereby reducing the risk of relapse. It typically involves psychoeducation — teaching family members about schizophrenia — alongside communication training and problem-solving skills. Studies have found that family therapy can reduce relapse rates by up to 50 percent in some cases. Token economy is a behaviour modification technique used in institutional settings. It operates on operant conditioning principles — patients are rewarded with tokens for exhibiting socially desirable behaviours, which they can exchange for privileges. It is most effective for managing negative symptoms in long-term care settings, but critics argue it does not address the underlying causes of schizophrenia and raises ethical concerns about autonomy. Now, exam tips and common mistakes. Let's talk about what costs students marks. Number one: confusing reliability and validity. Reliability refers to the consistency of diagnosis — would two different clinicians give the same patient the same diagnosis? Validity refers to the accuracy of diagnosis — does the diagnosis actually reflect the true nature of the disorder? These are completely different concepts, and mixing them up is one of the most common errors examiners see. Remember: Reliability equals Repeatability. Validity equals Veracity — truth. Number two: failing to be specific about neural correlates. Don't just write "there is too much dopamine" or "there are brain abnormalities." You need to specify which pathway, which brain region, and which symptom type. Ventral striatum hyperdopaminergia links to positive symptoms. Prefrontal cortex hypodopaminergia links to negative symptoms. Number three: presenting the schizophrenogenic mother or double bind theories without critical evaluation. Always acknowledge the lack of empirical support and the socially sensitive nature of these theories. Number four: in therapy questions, failing to distinguish between the mechanism of action and the therapeutic effect. For Chlorpromazine, the mechanism is D2 receptor blockade; the therapeutic effect is reduction of positive symptoms. These are different things, and examiners want to see both. Number five: for 16-mark discuss questions, remember the AO weighting. You should allocate approximately 6 marks worth of content to AO1 — description — and 10 marks worth to AO3 — evaluation. Many students write too much description and not enough evaluation. The interactionist approach — the diathesis-stress model — is your most sophisticated evaluative tool. Use it as a conclusion to biological or psychological explanation questions to show that neither approach alone is sufficient. Now for your quick-fire recall quiz. I'll ask the question — pause the podcast, think of your answer, then I'll give it to you. Question one: What is the difference between a hallucination and a delusion? Pause now. A hallucination is a sensory experience without an external stimulus. A delusion is a fixed false belief not amenable to reason. Question two: What does hyperdopaminergia in the mesolimbic pathway cause? Pause now. Positive symptoms — hallucinations and delusions. Question three: What was the concordance rate for schizophrenia in monozygotic twins according to Gottesman 1991? Pause now. Approximately 48 percent. Question four: What is the mechanism of action of Clozapine, and what makes it different from Chlorpromazine? Pause now. Clozapine blocks D2, D4, and serotonin receptors, reducing both positive and negative symptoms. Chlorpromazine primarily blocks D2 receptors and mainly reduces positive symptoms. Question five: What does CBTp stand for, and what is its primary aim? Pause now. Cognitive Behavioural Therapy for Psychosis. Its primary aim is to help patients identify and challenge distorted thinking patterns to reduce distress, not necessarily to eliminate symptoms. Let's wrap up. Today we've covered the classification of schizophrenia using DSM-5 and ICD-10, the distinction between positive and negative symptoms, the revised dopamine hypothesis with its two pathways, genetic and neural explanations, cognitive and family dysfunction psychological explanations, and the key therapies — typical and atypical antipsychotics, CBTp, family therapy, and token economy. We've also covered the interactionist diathesis-stress model, which is your most powerful evaluative framework. The key message to take away is this: schizophrenia is a complex disorder that cannot be fully explained by any single approach. The most sophisticated answers — the ones that get into the top mark bands — are those that acknowledge this complexity, use specific evidence to support and challenge each explanation, and conclude with the interactionist model as a synthesis. That's what separates a grade B from a grade A. Good luck with your revision. You've got this. See you in the next episode.
Key Terms & Definitions
- Reliability (in diagnosis)
- The consistency of a measuring instrument. In this context, the extent to which different clinicians agree on the same diagnosis for the same patient (inter-rater reliability).
- Validity (in diagnosis)
- The extent to which a test or diagnosis measures what it claims to measure. In this context, whether a diagnosis of schizophrenia is accurate and meaningful.
- Avolition
- A negative symptom of schizophrenia characterised by a lack of motivation or ability to initiate and persist in goal-directed behaviour.
- Diathesis-Stress Model
- An interactionist model which proposes that mental disorders develop from a genetic or biological predisposition for that illness (diathesis) combined with stressful conditions that play a precipitating or facilitating role (stress).
- Typical Antipsychotic
- A first-generation antipsychotic drug (e.g., Chlorpromazine) that works by blocking D2 dopamine receptors. Primarily effective for positive symptoms.
- Expressed Emotion (EE)
- A family communication style that involves high levels of criticism, hostility, and emotional over-involvement directed at a patient. It is a strong predictor of relapse.
Worked Examples
Worked Example
Question: Discuss biological explanations for schizophrenia. (16 marks)
Solution: **Introduction**: Biological explanations for schizophrenia focus on the roles of genetics, neurochemistry, and brain structure. The most prominent theories are the dopamine hypothesis, the genetic explanation supported by twin studies, and the identification of neural correlates such as enlarged ventricles. While there is strong evidence for a biological predisposition, a purely biological account is insufficient, and an interactionist approach is often preferred. **AO1 Paragraph 1 - The Dopamine Hypothesis**: The revised dopamine hypothesis posits that schizophrenia is caused by dopamine dysregulation in two key brain pathways. Hyperdopaminergia (excess dopamine) in the subcortical mesolimbic pathway is linked to positive symptoms like hallucinations. In contrast, hypodopaminergia (low dopamine) in the mesocortical pathway to the prefrontal cortex is linked to negative symptoms like avolition. This explains why different antipsychotics have varying effects. **AO3 Evaluation 1**: The dopamine hypothesis is supported by evidence from drugs. Leucht et al.'s (2013) meta-analysis of 212 studies found that all antipsychotics tested were significantly more effective than a placebo in reducing symptoms, lending strong support to the idea that dopamine is involved. However, the fact that antipsychotics are not effective for all patients and that it takes several weeks for them to work, despite blocking dopamine immediately, suggests that the neurochemical explanation is more complex than just dopamine levels. **AO1 Paragraph 2 - Genetic Explanation**: There is strong evidence for a genetic vulnerability. Gottesman (1991) found a 48% concordance rate in MZ twins, compared to 17% in DZ twins. As schizophrenia is polygenic, multiple genes, such as the COMT gene which is involved in dopamine regulation, have been identified as conferring a small increase in risk. **AO3 Evaluation 2**: The genetic explanation is a scientifically credible approach. However, the fact that the concordance rate for MZ twins is not 100% is a major limitation, proving that environmental factors must also play a role. This leads to the diathesis-stress model, which argues that a genetic vulnerability is triggered by an environmental stressor (e.g., childhood trauma or cannabis use). Therefore, the genetic explanation is incomplete on its own. **AO1 Paragraph 3 - Neural Correlates**: Neural correlates are structural and functional brain abnormalities associated with schizophrenia. For example, many patients have enlarged ventricles, suggesting a loss of brain tissue. Juckel et al. (2006) also identified a negative correlation between activity in the ventral striatum and the severity of negative symptoms. **AO3 Evaluation 3**: While the evidence for neural correlates is strong, the correlation-causation problem is a significant issue. It is unclear whether the brain abnormalities are a cause of schizophrenia or a consequence of the illness (or even the medication used to treat it). This limits the explanatory power of this line of research. **Conclusion**: In conclusion, biological explanations provide a robust and evidence-based account of the origins of schizophrenia. The dopamine hypothesis, in particular, has led to effective treatments. However, these explanations are biologically reductionist and determinist, ignoring the role of psychological and social factors. The most comprehensive explanation is the interactionist approach, which synthesises biological vulnerability with environmental triggers to provide a more complete and less deterministic picture of the disorder.
Worked Example
Question: Outline and evaluate one psychological therapy for schizophrenia. (8 marks)
Solution: **Outline (AO1)**: One psychological therapy for schizophrenia is Cognitive Behavioural Therapy for Psychosis (CBTp). The core assumption of CBTp is that symptoms are exacerbated by irrational beliefs. The therapy aims to help patients identify and challenge these beliefs. For example, a patient hearing voices might be encouraged to evaluate the content of the voices and consider alternative explanations for their origin (e.g., as a manifestation of their own anxiety). The therapist and patient work together to develop coping strategies to reduce the distress caused by the symptoms. CBTp does not aim to eliminate symptoms but to improve the patient's ability to function. **Evaluation (AO3)**: A major strength of CBTp is the evidence supporting its effectiveness. The NICE guidelines recommend CBTp for all patients with schizophrenia. Jauhar et al. (2014) conducted a meta-analysis and found that CBTp has a significant, albeit small, effect on both positive and negative symptoms. This provides good empirical support for its use. A further strength is that it empowers the patient by giving them control over their own recovery and teaching them skills that can be used long-term, unlike drug therapies which only work as long as they are taken. However, a significant limitation is that CBTp is not suitable for all patients. It requires a high level of motivation and the ability to engage in abstract thought, which can be very difficult for patients experiencing acute psychosis or severe negative symptoms like avolition. Furthermore, there are issues with availability, as there is often a shortage of trained therapists, meaning many patients who could benefit do not get access to the treatment.
Worked Example
Question: Jemima has been diagnosed with schizophrenia. She spends most of her day in bed, has stopped seeing her friends, and speaks in very short, empty sentences. Her doctor prescribes an antipsychotic drug. Referring to Jemima's behaviour, explain which type of antipsychotic would be most suitable for her. (4 marks)
Solution: Jemima is displaying negative symptoms of schizophrenia. Her spending most of her day in bed is evidence of **avolition** (lack of motivation). Her stopping seeing friends could be **social withdrawal**, and her short, empty sentences are characteristic of **alogia** (speech poverty). Therefore, an **atypical antipsychotic** (e.g., Clozapine or Risperidone) would be most suitable for her. This is because typical antipsychotics mainly treat positive symptoms and can even worsen negative symptoms. Atypical antipsychotics, however, act on both dopamine and serotonin receptors and are effective in treating both positive and negative symptoms, which would directly address Jemima's avolition and alogia.
Practice Questions
Question: Outline and evaluate the genetic explanation for schizophrenia. (8 marks)
Answer:
Question: Discuss psychological explanations for schizophrenia. (16 marks)
Answer:
Question: Apart from drug therapy, briefly outline one way of managing schizophrenia. (2 marks)
Answer:
Question: Explain the difference between typical and atypical antipsychotics. (4 marks)
Answer:
Question: Explain one limitation of using family dysfunction as an explanation for schizophrenia. (3 marks)
Answer: