Addictive Behaviours Revision Notes
Subject: Psychology | Level: A-Level | Exam Board: WJEC
This study guide provides a comprehensive analysis of Addictive Behaviours for the WJEC A-Level Psychology specification. It delves into the biological, psychological, and social explanations for addiction, equipping students with the detailed knowledge and critical evaluation skills required to achieve top marks.
Revision Notes & Key Concepts
Revision Podcast Transcript
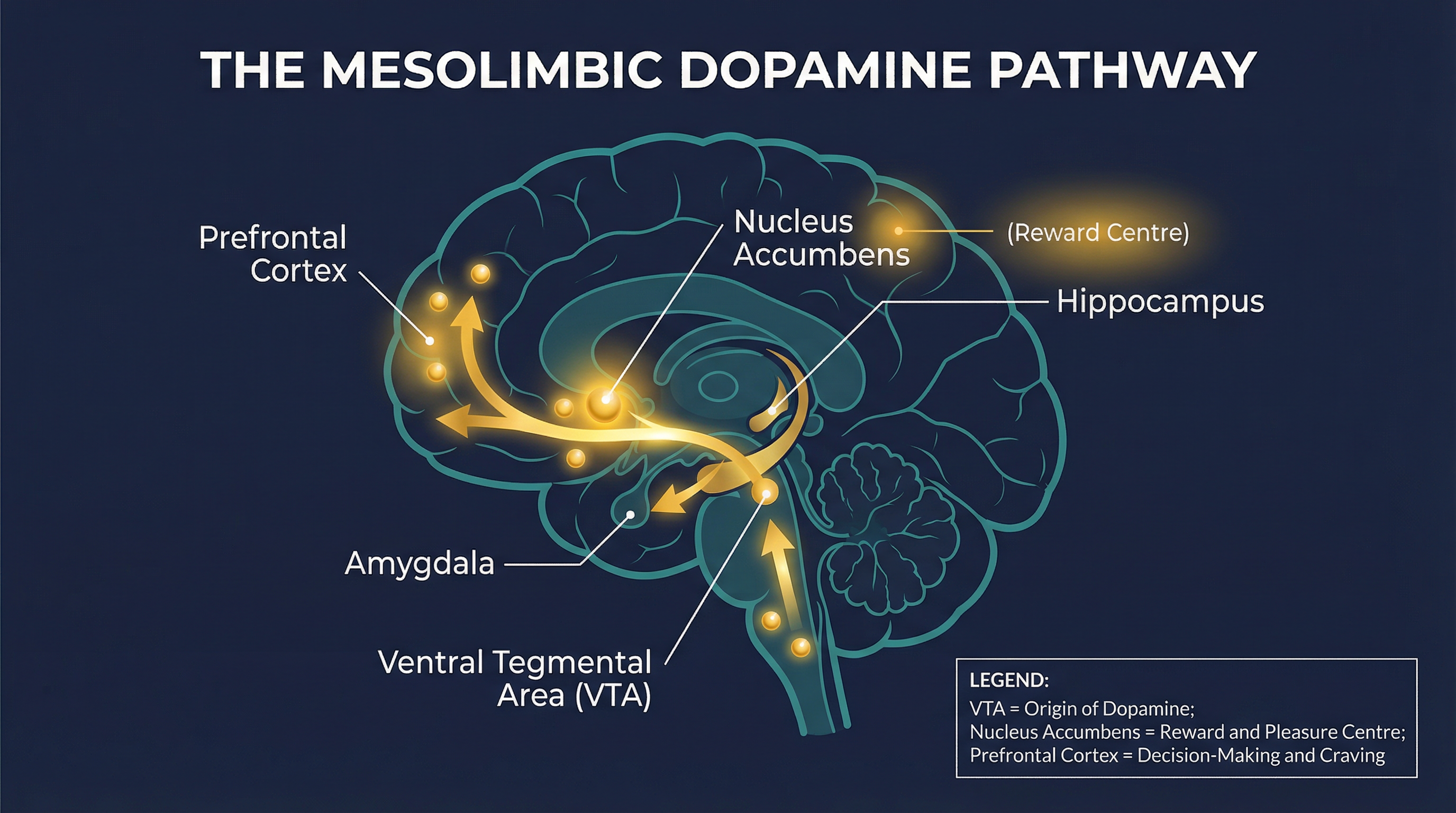
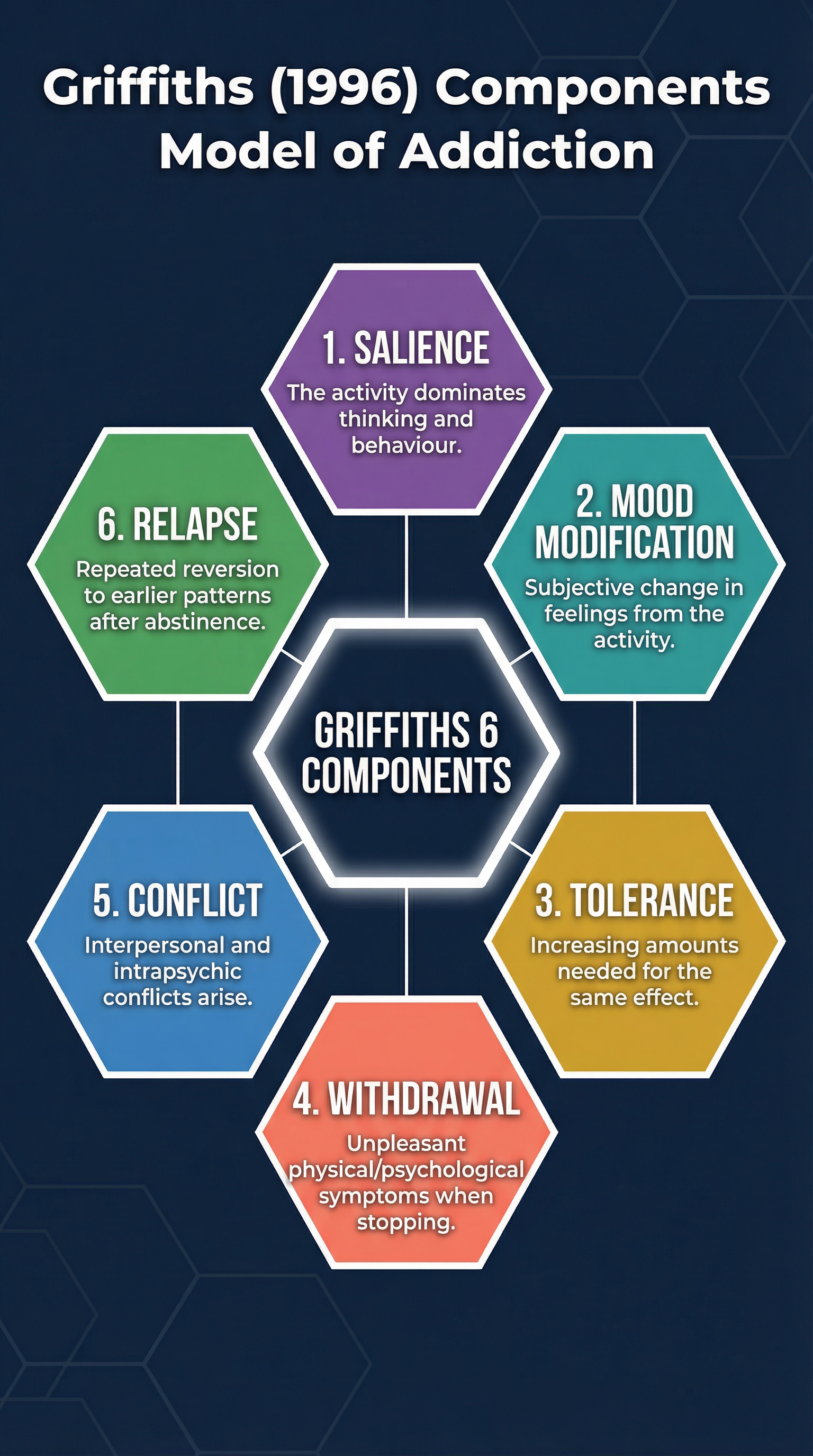
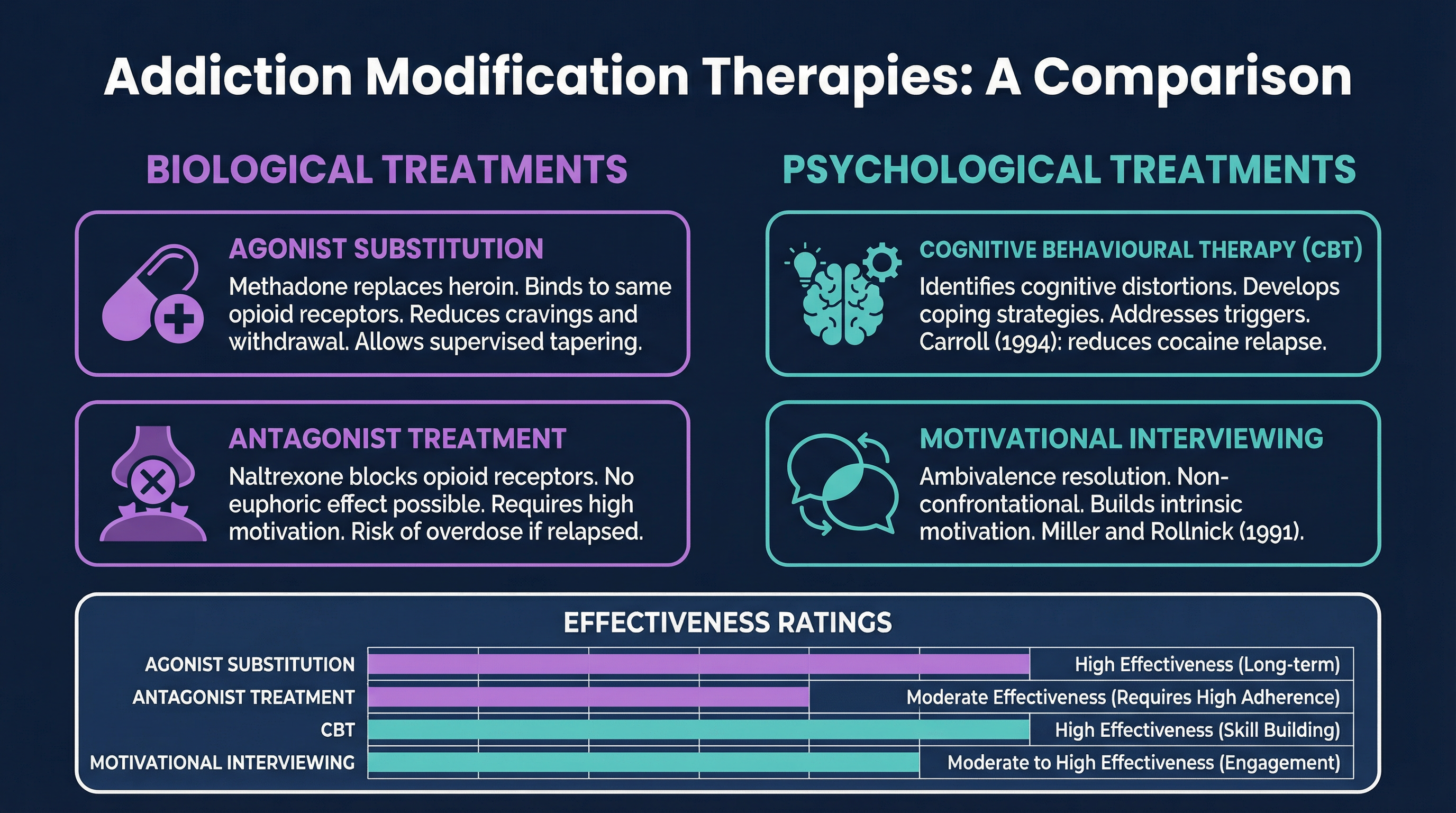
Welcome to PsychRevise — your go-to podcast for A-Level Psychology exam prep. I'm your host, and today we're diving deep into one of the most fascinating and clinically relevant topics on the WJEC specification: Addictive Behaviours. Whether you're sitting your exam in a few weeks or just starting to get to grips with this unit, this episode is going to walk you through everything you need to know — clearly, confidently, and with your mark scheme in mind. So grab a pen, get comfortable, and let's get started. Addictive Behaviours sits in Unit 3, Section A of the WJEC A-Level Psychology specification. It's a topic that brings together biological, psychological, and social explanations — and the examiners absolutely love to see candidates who can move fluently between all three levels of explanation. The assessment objective breakdown is important here: AO1 is worth 40 percent of your marks — that's your knowledge and understanding — but AO3, your evaluation and critical analysis, is worth a whopping 50 percent. So you need to do more than just describe. You need to evaluate, compare, and critically engage. Keep that in mind throughout everything we cover today. Let's start with the foundations. What actually is addiction? The most widely used framework in WJEC exams comes from Mark Griffiths, who in 1996 proposed his Components Model of Addiction. Griffiths argued that all addictions — whether to substances like heroin or alcohol, or to behaviours like gambling — share six core components. And you absolutely must know all six. Let me walk you through them. First: Salience. This is when the addictive activity becomes the most important thing in a person's life — it dominates their thinking, their feelings, and their behaviour. Even when they're not engaging in the activity, they're thinking about it. Second: Mood Modification. This refers to the subjective change in feelings that people experience when they engage in the addictive behaviour — it might be a buzz, a high, a sense of calm, or an escape. Third: Tolerance. Over time, the person needs more and more of the substance or behaviour to achieve the same effect. Think of a heroin user who needs increasingly larger doses to feel the same high. Fourth: Withdrawal. When the person stops or reduces the activity, they experience unpleasant physical or psychological symptoms — shaking, sweating, anxiety, irritability. These withdrawal symptoms are a key diagnostic indicator. Fifth: Conflict. This refers to the conflicts that arise as a result of the addiction — both interpersonal conflicts, like arguments with family and friends, and intrapsychic conflicts, meaning internal conflict and guilt within the person themselves. And sixth: Relapse. This is the tendency to return to earlier patterns of addictive behaviour after a period of abstinence — even after weeks, months, or years of being clean. A great memory hook for these six components is the acronym S-M-T-W-C-R: Salience, Mood Modification, Tolerance, Withdrawal, Conflict, Relapse. Or you can remember the phrase: "Some Monkeys Throw Wild Coconuts Repeatedly." Silly, but it works. Now let's move on to the biological explanation of addiction, because this is where the real exam marks live. The biological approach focuses on the role of neurochemistry — specifically the neurotransmitter dopamine — and the mesolimbic pathway in the brain. Here's how it works. Deep in the brain, in a region called the Ventral Tegmental Area — or VTA — dopamine-producing neurons fire in response to rewarding stimuli. These neurons send dopamine along a pathway to the Nucleus Accumbens, which is sometimes called the brain's reward centre. When dopamine floods the nucleus accumbens, we experience pleasure, motivation, and a sense of reward. This is completely normal — it happens when we eat, when we exercise, when we socialise. But addictive substances and behaviours hijack this system. Drugs like heroin, cocaine, and nicotine cause an abnormally large release of dopamine in the nucleus accumbens — far greater than any natural reward. Cocaine, for example, works by blocking the reuptake of dopamine at the synapse, meaning dopamine stays in the synaptic cleft for longer and continues to stimulate the postsynaptic receptor. The result is an intense, artificial high. The brain begins to associate the drug with extreme pleasure, and the mesolimbic pathway becomes sensitised to drug-related cues. This leads us to the desensitisation hypothesis, which is really important for WJEC. With repeated drug use, the brain actually reduces the number of dopamine receptors in the nucleus accumbens — a process called downregulation. This means the person needs more of the drug to achieve the same dopamine response — which explains tolerance. And when they stop using, dopamine activity falls below normal baseline levels — which explains the dysphoria and anhedonia of withdrawal. The person literally cannot feel pleasure from normal activities anymore. Now, how do we evaluate the biological explanation? This is where your AO3 marks come from. One strength is that the biological explanation is well-supported by neuroscientific research. Volkow and colleagues used PET scanning to demonstrate reduced dopamine D2 receptor availability in the striatum of cocaine users compared to non-users — providing objective, empirical support. However — and this is a critical evaluation point — the biological explanation is reductionist. And here's the key: don't just say it's reductionist. Explain why that matters. If we focus solely on dopamine and the mesolimbic pathway, we fail to account for why some people exposed to the same substances never become addicted, while others do. Social factors — like peer pressure, socioeconomic deprivation, and adverse childhood experiences — are powerful predictors of addiction that a purely biological account cannot explain. This links to the nature-nurture debate: addiction is best understood as an interaction between biological vulnerability and environmental triggers. Let's now look at psychological explanations. The learning theory account of addiction draws on both classical and operant conditioning. In classical conditioning, neutral stimuli — like the sight of a needle, a particular location, or even a smell — become conditioned stimuli that trigger cravings through their repeated association with the drug. This is why relapse is so common when people return to environments where they previously used. In operant conditioning, the drug use is positively reinforced by the pleasurable effects — the high — and negatively reinforced by the removal of withdrawal symptoms. This is a really common exam mistake, so listen carefully: negative reinforcement is NOT punishment. Negative reinforcement is when a behaviour is strengthened because it removes something unpleasant — in this case, taking heroin removes the painful withdrawal symptoms, which makes the person more likely to take heroin again. That is negative reinforcement. Social Learning Theory, developed by Bandura, adds another layer. People may initiate drug use through observation and imitation of role models — particularly peers or media figures — who appear to gain status or pleasure from the behaviour. Vicarious reinforcement plays a key role here. Cognitive explanations focus on the role of irrational beliefs and cognitive biases. Beck and colleagues identified that addicted individuals often hold distorted beliefs about their ability to control their use — "I can stop whenever I want" — and about the necessity of the substance — "I need this to cope." These cognitive distortions maintain the addiction and are a key target for CBT. Now let's talk about treatments — because the exam loves to ask you to evaluate modification therapies. There are two main categories: biological and psychological. Starting with biological treatments. Agonist substitution involves replacing the addictive substance with a safer substitute that acts on the same receptors. The classic example is methadone for heroin addiction. Methadone is a synthetic opioid that binds to the same mu-opioid receptors as heroin, but it has a longer half-life, produces less euphoria, and can be administered in controlled doses. This reduces cravings and withdrawal symptoms, allowing the person to stabilise their life. Research by Mattick and colleagues in a 2009 Cochrane review found that methadone maintenance was significantly more effective than no treatment in retaining patients in treatment and reducing heroin use. However, methadone is itself addictive, and there are ethical concerns about simply substituting one dependency for another. Antagonist treatments work differently. Naltrexone, for example, blocks opioid receptors entirely — it occupies the receptor without activating it, so if the person takes heroin, they feel no effect. This removes the positive reinforcement of drug use. However, naltrexone requires extremely high motivation from the patient, and there is a serious risk: if a person relapses after a period of abstinence, their tolerance will have dropped significantly. If they then take the same dose they used before, they risk fatal overdose. Moving to psychological treatments. Cognitive Behavioural Therapy, or CBT, is one of the most evidence-based treatments for addiction. It works by identifying and challenging the cognitive distortions that maintain addictive behaviour, and by developing practical coping strategies for managing triggers and cravings. Carroll and colleagues in 1994 conducted a randomised controlled trial with cocaine users and found that CBT significantly reduced cocaine use compared to a control group, with effects that were maintained at 12-month follow-up. A key strength of CBT is that it addresses the underlying psychological mechanisms rather than just the symptoms — it gives people transferable skills. However, CBT requires significant time commitment and cognitive engagement, which may not be accessible to all patients, particularly those with severe addiction or comorbid mental health conditions. Now, let me give you your exam tips and common mistakes section — this is where you can really pick up marks. Tip one: when you're asked to evaluate a treatment or explanation, always use the PEEL structure. Point — state your evaluative point clearly. Evidence — name a specific study with researcher and date. Explain — explain what the study found and why it supports or challenges the explanation. Link — connect it back to the question. Generic points like "it is reductionist" or "it ignores free will" will only get you into the lower mark bands. You need to contextualise every evaluation point to addiction specifically. Tip two: always name the neurotransmitter AND the brain region. Don't just say "dopamine is released." Say "dopamine is released from the Ventral Tegmental Area and travels along the mesolimbic pathway to the Nucleus Accumbens." That level of specificity is what separates Level 3 from Level 4 answers. Tip three: when applying learning theories, always distinguish between initiation, maintenance, and relapse. Classical conditioning best explains why cues trigger relapse. Operant conditioning best explains maintenance — the ongoing cycle of use. Social Learning Theory best explains initiation — why someone first tries a substance. Examiners credit candidates who make these distinctions explicitly. Tip four: use Issues and Debates as an evaluative framework, but make sure they're contextualised. Don't just say "this is deterministic." Say: "The biological explanation is deterministic because it suggests that once the mesolimbic pathway has been hijacked by drug use, the individual has limited control over their behaviour. This raises ethical concerns about how we treat addicted individuals — are they morally responsible, or are they victims of their neurochemistry? This has implications for policy and treatment." Tip five: time management. For a 10-mark Describe question, allocate 15 minutes. For a 15-mark Evaluate question, allocate 25 minutes. Don't spend all your time on description — the AO3 marks are where the majority of the credit lies. Now let's do a quick-fire recall quiz. I'll ask a question — pause the podcast, think of your answer, then I'll give you the key points. Ready? Question one: Name all six of Griffiths' components of addiction. Pause now. The answer is: Salience, Mood Modification, Tolerance, Withdrawal, Conflict, Relapse. Remember: Some Monkeys Throw Wild Coconuts Repeatedly. Question two: What is the role of the Nucleus Accumbens in addiction? Pause now. It is the brain's reward centre, located in the mesolimbic pathway. Dopamine floods the nucleus accumbens in response to rewarding stimuli, including addictive drugs, producing feelings of pleasure and reinforcing drug-seeking behaviour. Question three: What is the difference between agonist substitution and antagonist treatment? Pause now. Agonist substitution — like methadone — activates the same receptors as the addictive drug, reducing cravings and withdrawal. Antagonist treatment — like naltrexone — blocks the receptors, preventing the drug from having any effect. Question four: Why is negative reinforcement important in explaining addiction maintenance? Pause now. Negative reinforcement occurs when a behaviour is strengthened by the removal of an unpleasant stimulus. In addiction, taking the drug removes withdrawal symptoms — which are deeply unpleasant — thereby reinforcing drug-taking behaviour and making it more likely to recur. And that brings us to our summary and sign-off. Today we've covered the key foundations of Addictive Behaviours for WJEC A-Level Psychology. We've looked at Griffiths' six components model, the biological explanation centred on dopamine and the mesolimbic pathway, the desensitisation hypothesis, learning theory accounts including classical conditioning, operant conditioning, and social learning theory, cognitive explanations, and modification therapies including methadone, naltrexone, and CBT. We've also covered the most common exam mistakes and how to structure your evaluation using PEEL. The most important thing to remember is this: your AO3 marks are 50 percent of the total. Every evaluation point needs a named study, a specific explanation, and a link back to the question. Generic evaluation will not get you into the top mark band. Good luck with your revision. You've got this. I'll see you in the next episode of PsychRevise.
Key Terms & Definitions
- Addiction
- A state of psychological and/or physical dependence on a substance or activity, characterised by a compulsive need to engage in the behaviour despite negative consequences.
- Tolerance
- The process whereby the body adapts to a substance, requiring increasingly larger doses to achieve the same physiological and psychological effects.
- Withdrawal
- A set of unpleasant physical and psychological symptoms experienced when a person abruptly stops or reduces their intake of a substance they are dependent on.
- Negative Reinforcement
- The strengthening of a behaviour because it leads to the removal or avoidance of an aversive (unpleasant) stimulus.
- Agonist
- A drug that binds to and activates a receptor in the brain, mimicking the effect of a natural neurotransmitter or another drug.
- Antagonist
- A drug that binds to a receptor in the brain but does not activate it, thereby blocking the receptor from being activated by other substances.
Worked Examples
Worked Example
Question: Describe and evaluate the biological explanation of addiction. (16 marks)
Solution: **Introduction**: The biological explanation frames addiction as a brain disease, focusing on neurochemical and genetic factors. The key mechanism is the effect of addictive substances on the mesolimbic dopamine pathway, which is central to reward and motivation. **Paragraph 1 - Description (AO1)**: The mesolimbic pathway involves the Ventral Tegmental Area (VTA) releasing dopamine to the Nucleus Accumbens (NAcc). Addictive drugs cause an abnormally large dopamine surge, creating intense pleasure. Over time, this leads to neuroadaptation, such as the downregulation of D2 receptors (the desensitisation hypothesis), which explains tolerance and withdrawal. **Paragraph 2 - Evaluation (AO3)**: A major strength is the wealth of supporting evidence from neuroscience. For example, **Volkow et al. (1997)** used PET scans to demonstrate reduced D2 receptor levels in the brains of cocaine addicts compared to controls. This provides objective, empirical evidence for the desensitisation hypothesis, increasing the scientific credibility of the explanation. **Paragraph 3 - Evaluation (AO3)**: However, the biological explanation is often criticised for being **reductionist**. By focusing solely on neurochemistry, it ignores the significant role of psychological and social factors. For instance, it cannot explain why some individuals with a supposed genetic vulnerability never develop an addiction, while others with no family history do. A more holistic, **diathesis-stress** model, which proposes that a biological predisposition is triggered by environmental stressors, offers a more complete explanation. **Paragraph 4 - Evaluation (AO3)**: A further issue is that much of the research is **correlational**. For example, while studies show a link between low D2 receptor levels and addiction, it is difficult to establish cause and effect. It is possible that low receptor levels are a pre-existing vulnerability factor, rather than a consequence of drug use. This ambiguity limits the conclusions we can draw about the causal role of dopamine in addiction. **Conclusion**: In conclusion, while the biological explanation provides a powerful and scientifically credible account of the mechanisms of tolerance and withdrawal, it is incomplete. Its reductionist and deterministic nature means it overlooks the crucial role of individual differences, cognition, and social context. A comprehensive understanding of addiction requires an interactionist approach.
Worked Example
Question: Using your knowledge of learning theory, explain how a person might develop and maintain a gambling addiction. (8 marks)
Solution: **Introduction**: Learning theory would explain a gambling addiction through a combination of classical and operant conditioning, as well as social learning. **Paragraph 1 - Initiation (SLT)**: Initiation can be explained by Social Learning Theory. An individual might observe a role model, such as a parent or peer, winning money and enjoying the social status that comes with it. This acts as **vicarious reinforcement**, motivating the individual to imitate the behaviour and try gambling for themselves. **Paragraph 2 - Maintenance (Operant Conditioning)**: Maintenance is primarily explained by operant conditioning. The occasional and unpredictable nature of winning money acts as a powerful **positive reinforcer** on a **variable-ratio schedule of reinforcement**. This schedule is highly resistant to extinction, keeping the person gambling even during long losing streaks. Furthermore, the 'buzz' and excitement of the gambling environment can act as a negative reinforcer, providing an escape from stress or boredom. **Paragraph 3 - Relapse (Classical Conditioning)**: Relapse can be explained by classical conditioning. Environmental cues associated with gambling, such as the sound of a slot machine, the bright lights of an arcade, or even the notification from a betting app, become **conditioned stimuli**. These cues can trigger intense cravings and a physiological arousal response, leading a person to relapse even after a period of abstinence.
Worked Example
Question: Evaluate the use of agonist substitution as a treatment for addiction. (10 marks)
Solution: **Introduction**: Agonist substitution, such as methadone for heroin addiction, is a biological therapy that involves replacing a harmful addictive drug with a safer alternative that has a similar pharmacological action. Its effectiveness and ethics are subject to debate. **Paragraph 1 - Strength (Effectiveness)**: One major strength is its effectiveness in reducing harm and retaining patients in treatment. A Cochrane review by **Mattick et al. (2009)** found that methadone maintenance treatment was significantly more effective than placebo or no treatment in reducing illicit opioid use and retaining patients. By stabilising patients and reducing the chaos of street heroin use, it allows them to engage with other psychological therapies and improve their health and social stability. **Paragraph 2 - Weakness (Ethical Issues)**: However, a significant ethical criticism is that agonist substitution simply replaces one addiction with another. Patients become dependent on methadone, which also has a difficult withdrawal syndrome. Critics argue this does not address the root causes of addiction and can be seen as a form of social control, particularly as it is often administered in a highly regulated clinical setting. This raises questions about patient autonomy and the ultimate goal of treatment. **Paragraph 3 - Weakness (Side Effects & Limitations)**: Another limitation is the presence of side effects, which can include sedation, constipation, and sweating. Furthermore, there is a significant black market for methadone, and diverted doses can lead to overdose deaths in non-tolerant individuals. This highlights the risks associated with the treatment and the need for strict supervision, which can be costly and resource-intensive. **Conclusion**: In conclusion, agonist substitution is a highly effective harm reduction strategy with a strong evidence base. It saves lives and provides a platform for recovery. However, its ethical implications and the problem of substituting one dependency for another mean it is not a complete solution and should ideally be used as part of a wider, integrated treatment package that includes psychological support.
Practice Questions
Question: Describe the role of dopamine in the process of addiction. (6 marks)
Answer:
Question: Evaluate learning theory as an explanation for addiction. (10 marks)
Answer:
Question: Distinguish between agonist and antagonist treatments for addiction. (4 marks)
Answer:
Question: Explain one ethical issue related to the use of aversion therapy to treat addiction. (4 marks)
Answer:
Question: Outline Griffiths' (1996) six components of addiction. (6 marks)
Answer: