Biological Approach: Therapy Revision Notes
Comprehensive revision notes for WJEC A-Level.
Summary & Overview
This study guide provides a comprehensive overview of Psychosurgery for WJEC A-Level Psychology, tracing its controversial history from the 'ice-pick' lobotomy to modern, precise Deep Brain Stimulation. It is designed to equip candidates with the specific knowledge and evaluation skills needed to achieve top marks.
Study Material
## Overview
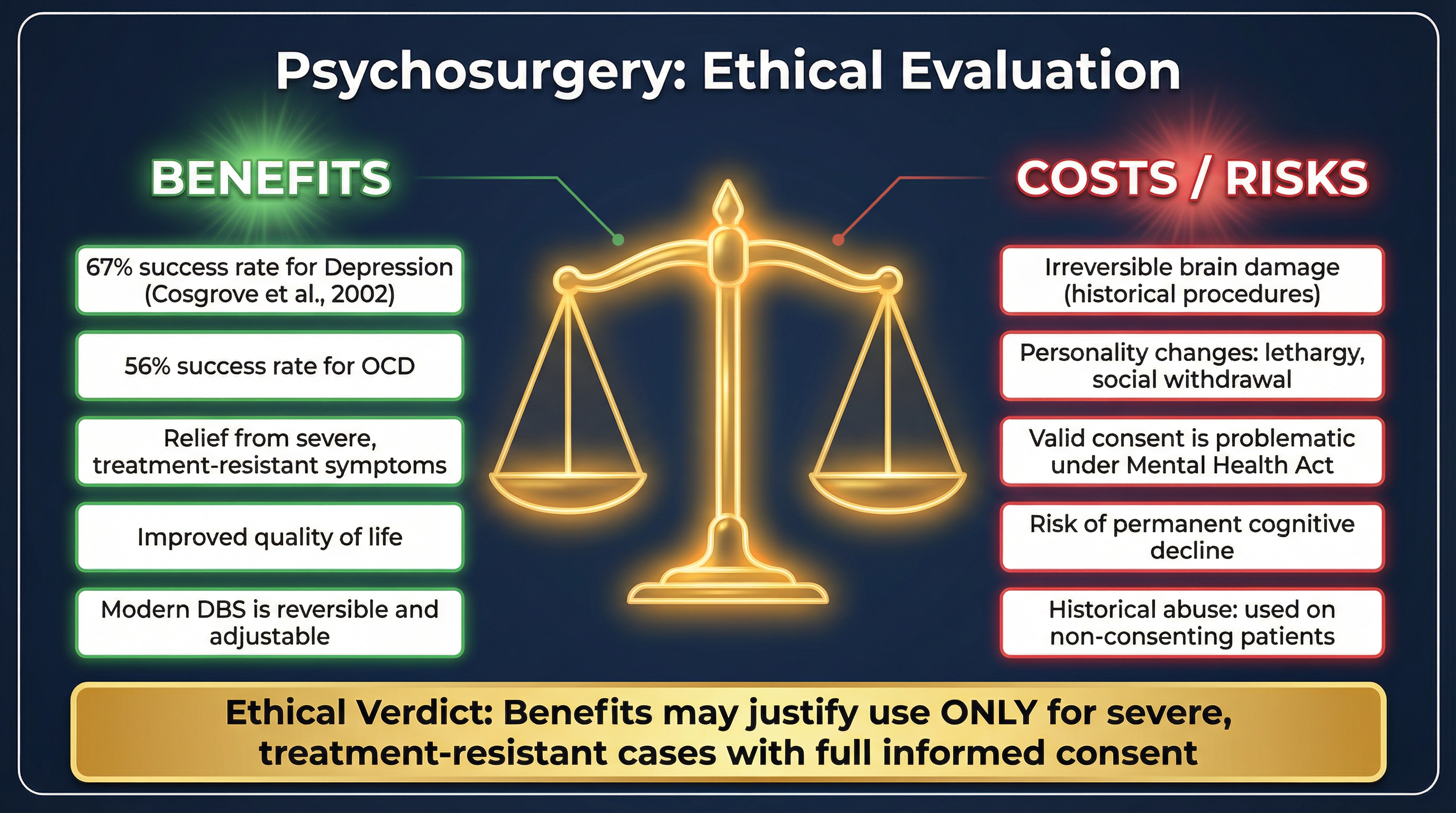
Psychosurgery is a critical and often misunderstood topic within the Biological Approach for WJEC A-Level Psychology. Examiners expect candidates to demonstrate a clear understanding of its historical trajectory, the distinction between early, crude procedures and modern, precise techniques, and a nuanced evaluation of its effectiveness and ethical implications. This guide will cover the key developments from Moniz's prefrontal leucotomy to stereotactic procedures and Deep Brain Stimulation (DBS). Credit is awarded for accurate descriptions of these procedures (AO1), balanced evaluation of their use with reference to specific evidence like Cosgrove et al. (AO3), and the ability to link the therapy back to core biological assumptions such as Localisation of Function. Candidates must avoid common pitfalls like conflating psychosurgery with ECT and provide specific, evidence-based ethical analysis rather than generic criticism.

## Key Events & Developments
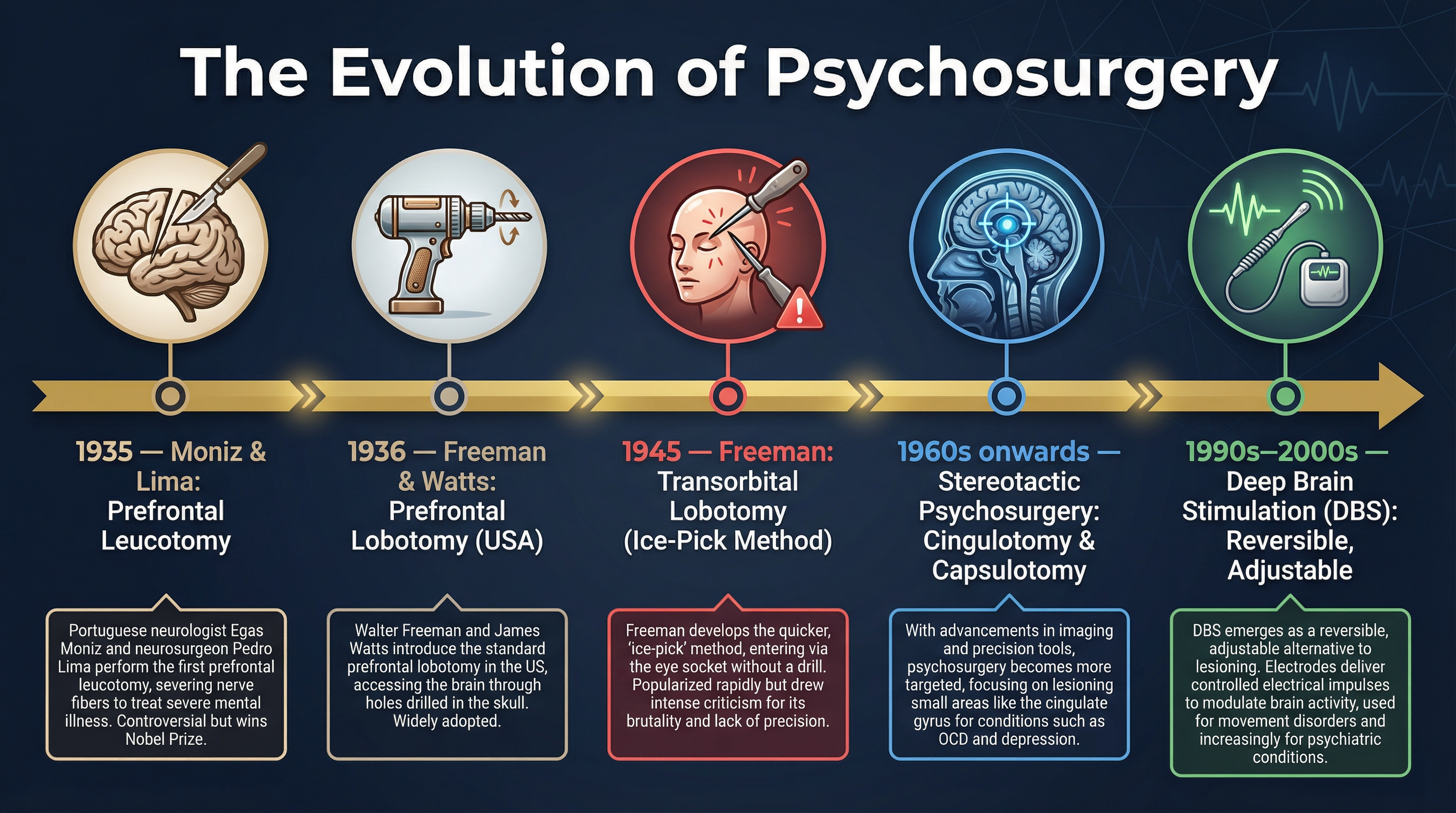
### Prefrontal Leucotomy
**Date(s)**: 1935
**What happened**: Portuguese neurologist Egas Moniz, with neurosurgeon Pedro Lima, performed the first prefrontal leucotomy. The procedure involved drilling holes into the patient's skull and using a leucotome (a wire loop instrument) to sever nerve fibres connecting the prefrontal cortex to deeper brain structures.
**Why it matters**: This marked the beginning of modern psychosurgery. It was the first systematic attempt to treat mental illness by surgically altering the brain, based on the assumption that faulty neural connections caused psychological distress. Moniz won the Nobel Prize for this in 1949, lending it significant, though controversial, credibility.
**Specific Knowledge**: Egas Moniz, Pedro Lima, leucotome, severing of prefrontal cortex fibres.
### Transorbital Lobotomy
**Date(s)**: From 1945
**What happened**: American neurologist Walter Freeman developed and popularised the transorbital lobotomy, a faster and more brutal procedure that did not require a traditional operating theatre. An instrument similar to an ice pick (an orbitoclast) was inserted through the top of the eye socket, piercing the thin bone with a tap from a mallet. The instrument was then swept back and forth to sever connections in the frontal lobes.
**Why it matters**: This procedure represents the peak of psychosurgery's use and also its most infamous chapter. Tens of thousands were performed, often on patients without their consent and with devastating side effects, including profound personality changes (passivity, apathy), cognitive deficits, and even death. It highlighted the severe ethical problems of 'blind' surgery.
**Specific Knowledge**: Walter Freeman, orbitoclast, 'ice-pick' method, lack of anaesthesia (sometimes only ECT), severe side effects.
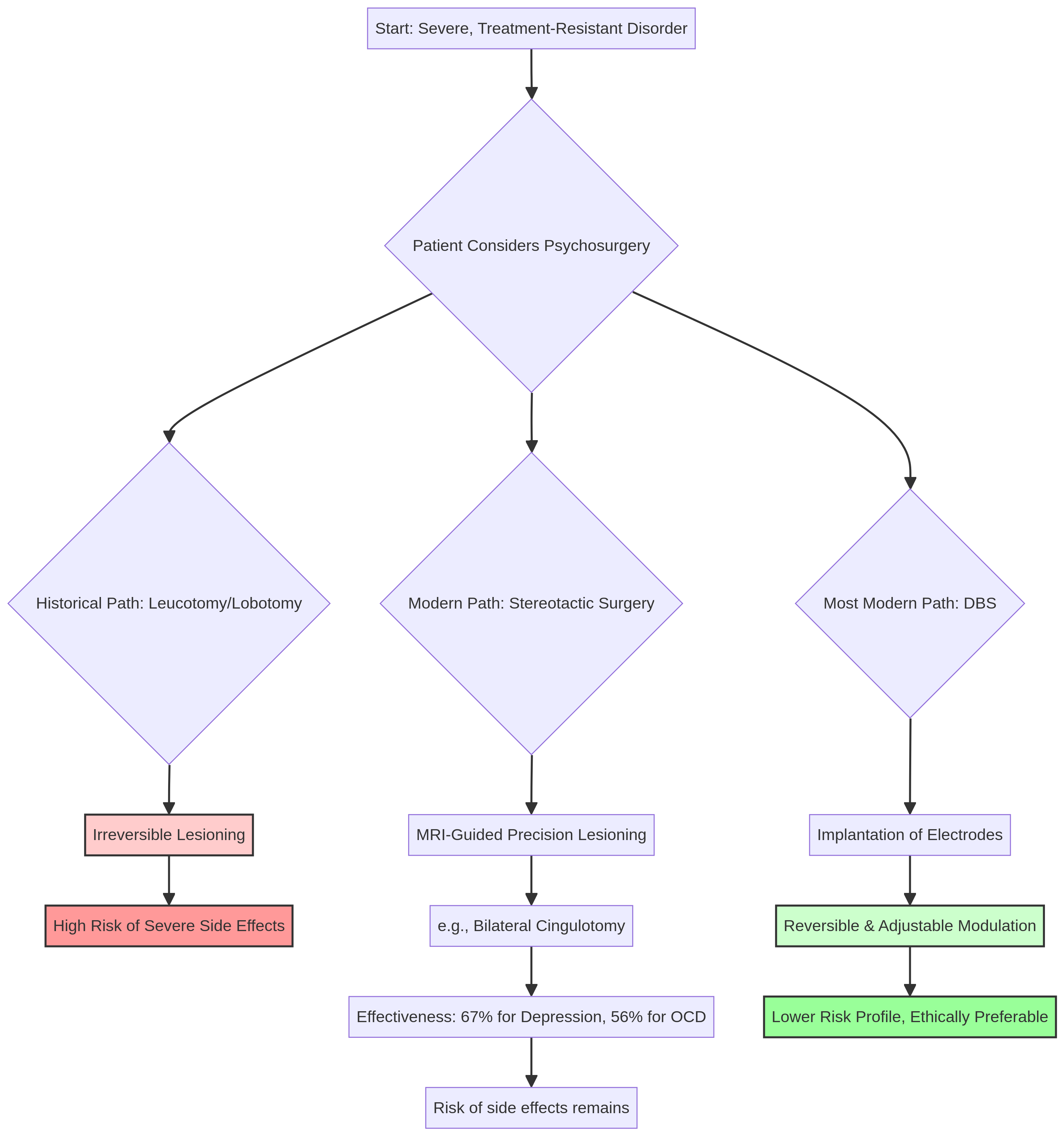
### Stereotactic Psychosurgery
**Date(s)**: 1960s onwards
**What happened**: With the advent of advanced neuroimaging techniques like MRI, psychosurgery became far more precise. Stereotactic procedures use a 3D coordinate system, guided by brain scans, to target specific, tiny areas of the brain for lesioning. This allows for much smaller, more accurate interventions.
**Why it matters**: This marked a crucial shift from 'blind' destruction to targeted therapy. It dramatically reduced the risk of catastrophic side effects and improved the potential for positive outcomes. For the WJEC exam, this demonstrates the critical evolution and refinement of the technique.
**Specific Knowledge**: MRI guidance, stereotactic frame, bilateral cingulotomy (targeting the cingulate gyrus for depression/OCD), anterior capsulotomy (targeting the internal capsule).
### Deep Brain Stimulation (DBS)
**Date(s)**: 1990s onwards
**What happened**: DBS is the most modern form of psychosurgery and involves implanting fine electrodes into specific brain regions. These electrodes are connected to a pulse generator (like a pacemaker) implanted in the chest, which delivers continuous electrical stimulation to modulate brain activity.
**Why it matters**: DBS is a revolutionary step because it is **reversible and adjustable**. Unlike lesioning procedures, no brain tissue is permanently destroyed. If a patient experiences negative side effects, the stimulation can be turned down or switched off. This fundamentally changes the ethical calculation, making it a much safer and more defensible intervention for treatment-resistant disorders.
**Specific Knowledge**: Electrodes, pulse generator, modulation of brain activity, reversibility, adjustability, used for depression and OCD.
## Key Individuals
### Egas Moniz
**Role**: Portuguese Neurologist, Nobel Prize Laureate
**Key Actions**: Pioneered the prefrontal leucotomy in 1935, attempting to sever neural pathways in the frontal lobes to alleviate symptoms of mental illness.
**Impact**: Considered the father of modern psychosurgery. His work, though now seen as crude and dangerous, established the principle of treating psychological disorders through direct brain intervention. His Nobel Prize gave the field a controversial legitimacy.
### Walter Freeman
**Role**: American Neurologist and Prolific Lobotomist
**Key Actions**: Adapted and aggressively popularised the lobotomy in the US, developing the transorbital ('ice-pick') method. He performed thousands of procedures, often with little regard for patient consent or aftercare.
**Impact**: Freeman is the figure most associated with the horrors of early psychosurgery. His showmanship and the sheer volume of his operations led to a public backlash and the eventual decline of the procedure. He serves as a key case study in medical ethics.
## Second-Order Concepts
### Causation
Psychosurgery was developed due to a combination of factors: the lack of any other effective treatments for severe mental illness in the early 20th century, the rise of the biological model of psychopathology (specifically the assumption of Localisation of Function), and the ambition of figures like Moniz and Freeman. The decline of early methods was caused by the development of the first effective antipsychotic and antidepressant drugs in the 1950s, coupled with growing public and medical concern over the severe side effects and ethical abuses.
### Consequence
The immediate consequences of early psychosurgery were often catastrophic: high rates of mortality and severe personality changes. The long-term consequence was a deep public and medical distrust of the procedure. However, a positive long-term consequence of this backlash was the development of much stricter ethical guidelines for medical research and the drive towards more precise, less invasive techniques like stereotactic surgery and DBS.
### Change & Continuity
The major **change** is the shift from indiscriminate destruction of brain tissue to precise, targeted, and even reversible modulation. The **continuity** is the underlying principle: that psychological disorders can be treated by intervening directly with the physical brain, an idea that stems directly from the core assumptions of the Biological Approach.
### Significance
Psychosurgery is historically significant because it represents one of the most extreme applications of the biological model. Its story is a powerful lesson in medical ethics, the importance of scientific rigour, and the dangers of treatments outpacing the understanding of the organ they target. For the exam, its significance lies in its ability to provide a rich topic for AO3 evaluation.
## Source Skills
When presented with a source on psychosurgery, candidates should first identify its nature. Is it a primary account from a patient or surgeon from the 1940s? Or a modern academic review? The provenance is key. A 1940s source is useful for understanding contemporary attitudes but will be limited by its lack of modern scientific understanding. A modern source is useful for its scientific accuracy but may lack insight into the historical context. Always evaluate what the source says (content), who created it and why (provenance), and what it cannot tell you (limitations).