Health Contributions and Effects of Exercise — WJEC A-Level Study Guide
Exam Board: WJEC | Level: A-Level
This guide provides a comprehensive analysis of the health contributions and effects of exercise, focusing on how physical activity mitigates hypokinetic diseases. It is tailored for the WJEC A-Level Physical Education specification, equipping candidates with the precise physiological knowledge and exam technique required to achieve top marks.
## Overview
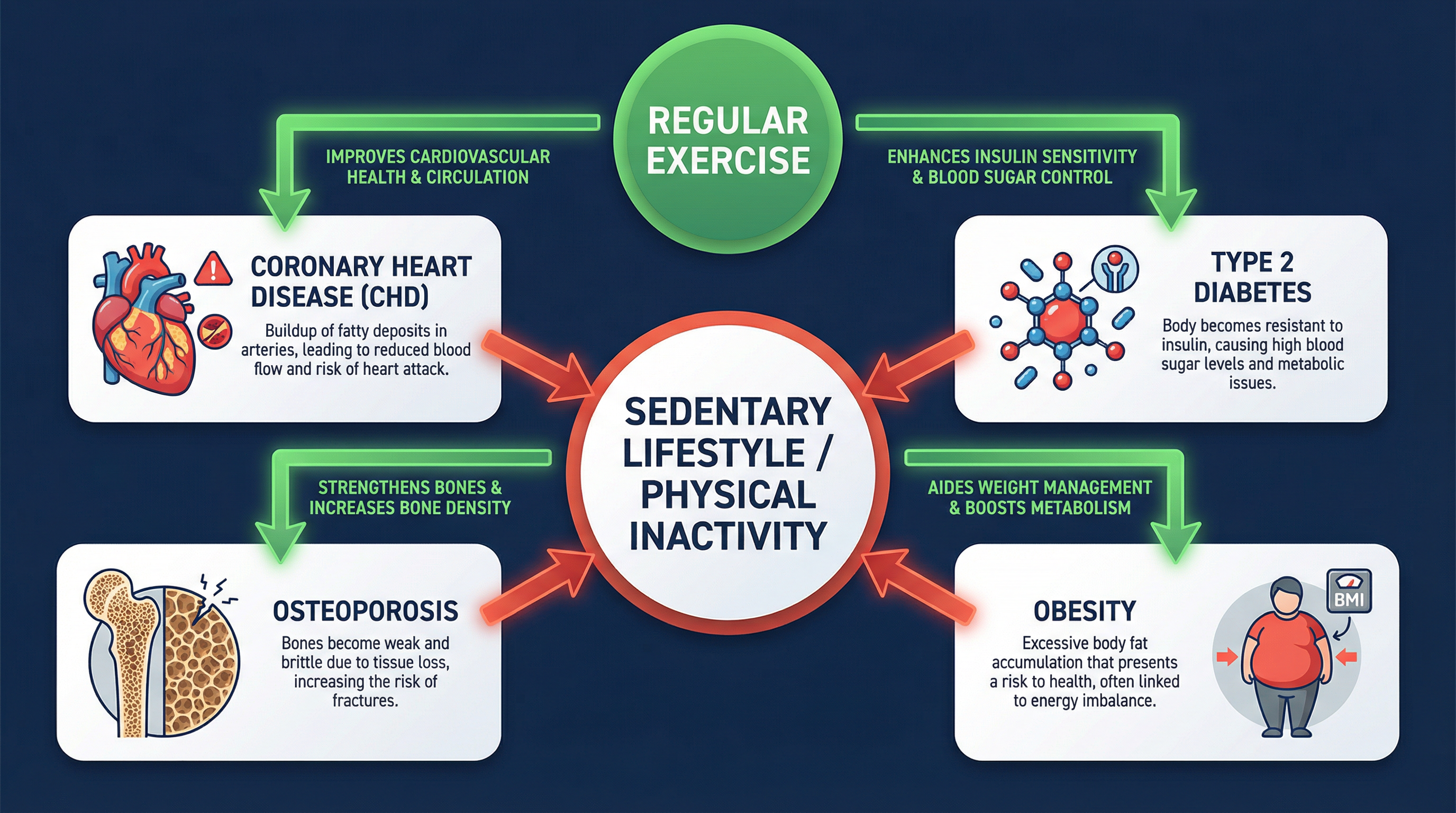
This unit explores the critical relationship between physical activity and long-term health, a cornerstone of the WJEC A-Level PE specification. Candidates are required to move beyond a general appreciation of exercise and develop a detailed understanding of the physiological and psychological mechanisms by which regular physical activity prevents and manages a range of **hypokinetic diseases** — conditions resulting from a sedentary lifestyle. A strong grasp of this topic is essential for success in the written exam, as it tests knowledge (AO1), application (AO2), and analysis (AO3) in depth.
## Key Knowledge & Theory
### Core Concepts
The central theme is how chronic (long-term) adaptation to exercise provides a protective effect against major health issues. Candidates must be able to explain the specific pathways through which exercise impacts the cardiovascular, metabolic, musculoskeletal, and endocrine systems.
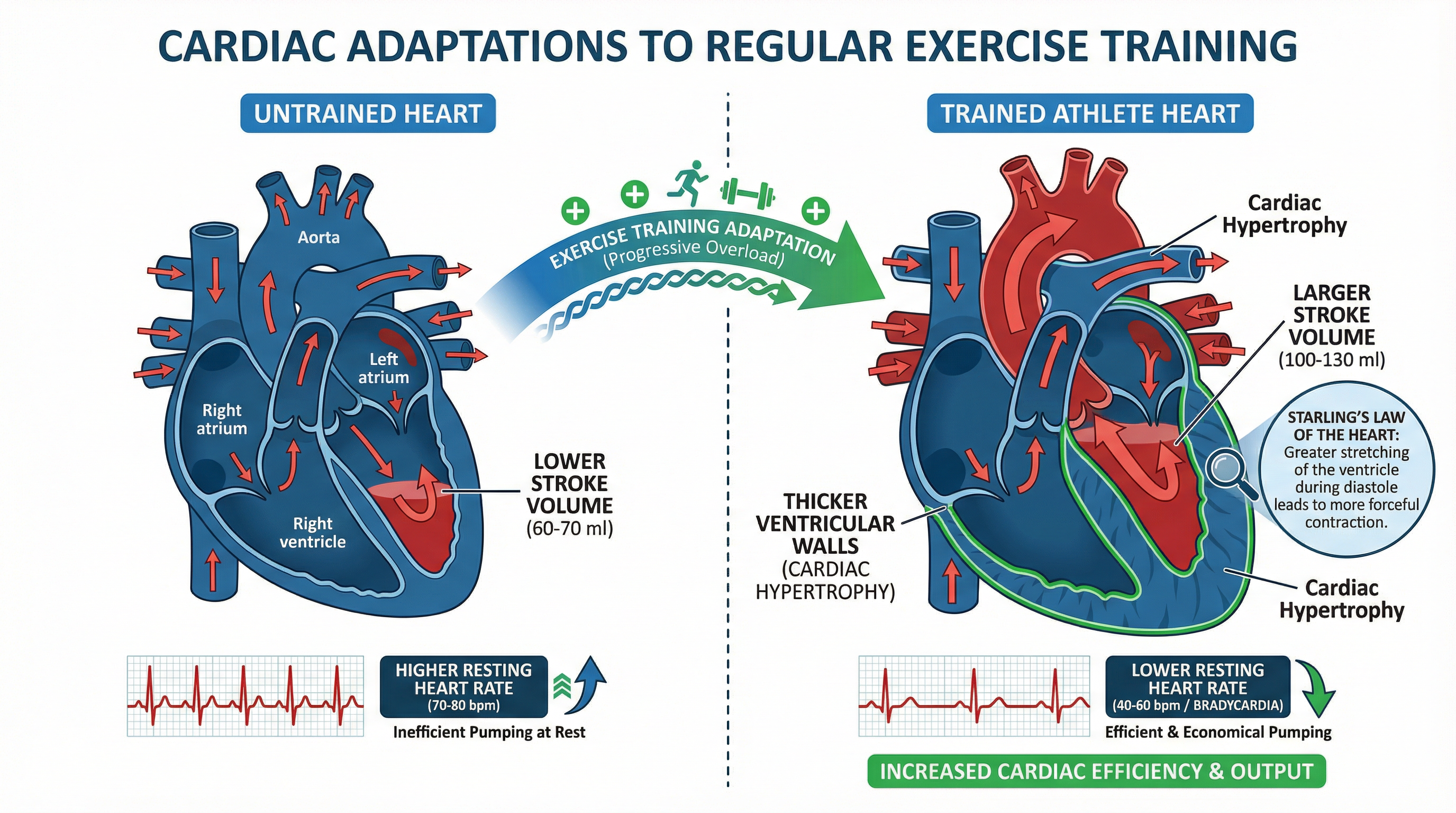
**1. Coronary Heart Disease (CHD) and Cardiovascular Adaptations:**
- **Cardiac Hypertrophy:** Regular aerobic exercise leads to the thickening of the heart's muscular wall, particularly the left ventricle. This is a positive adaptation that increases the heart's pumping capacity.
- **Increased Stroke Volume:** As the heart becomes stronger, it can pump more blood with each beat. This is known as an increased stroke volume.
- **Bradycardia:** A direct consequence of increased stroke volume is a lower resting heart rate. An efficient heart doesn't need to beat as often to supply the body with oxygenated blood. A resting heart rate below 60 bpm is termed bradycardia and is common in trained athletes.
- **Improved Lipid Profile:** Exercise positively alters blood cholesterol levels. It increases **High-Density Lipoproteins (HDL)**, often called 'good cholesterol', which transport cholesterol away from the arteries. Simultaneously, it decreases **Low-Density Lipoproteins (LDL)**, or 'bad cholesterol', which contribute to the formation of atherosclerotic plaques.
- **Increased Elasticity of Arterial Walls:** Exercise helps maintain the flexibility of blood vessels, which aids in regulating blood pressure and reducing the strain on the heart.
**2. Obesity and Energy Balance:**
- **Energy Balance Equation:** The fundamental principle is that weight is managed by balancing energy intake (calories from food) with energy expenditure (calories burned).
- **Increased Basal Metabolic Rate (BMR):** Exercise, particularly resistance training, builds muscle mass. Muscle tissue is more metabolically active than fat tissue, meaning it burns more calories even at rest, thus increasing BMR.
- **Excess Post-Exercise Oxygen Consumption (EPOC):** Following a bout of intense exercise, the body's metabolism remains elevated for several hours, continuing to burn calories at a higher rate. This 'afterburn' effect is a significant contributor to overall energy expenditure.
**3. Type 2 Diabetes and Glucose Regulation:**
- **Increased Insulin Sensitivity:** Type 2 diabetes is characterized by the body's cells becoming resistant to insulin. Exercise makes muscle cells more sensitive to insulin.
- **GLUT-4 Translocation:** During physical activity, muscle contractions stimulate the movement of glucose transporters, known as **GLUT-4**, to the cell surface. This allows glucose to be taken up by the muscles for energy, without relying on insulin. This is a crucial mechanism for controlling blood sugar levels.
**4. Osteoporosis and Bone Health:**
- **Osteoblastic Activity:** Osteoblasts are cells that build new bone tissue. **Weight-bearing and high-impact exercise** (e.g., running, gymnastics, resistance training) places stress on the skeleton, which stimulates osteoblasts to increase bone mineral density.
- **Specificity of Exercise:** It is vital to note that not all exercise builds bone. Non-weight-bearing activities like swimming or cycling, while excellent for cardiovascular health, have minimal impact on bone density.
### Technical Vocabulary
Using precise terminology is non-negotiable for achieving high marks. Candidates must be fluent in the following terms:
- **Hypokinetic Disease:** A disease associated with a sedentary or inactive lifestyle.
- **Atherosclerosis:** The build-up of fatty plaques within the arterial walls.
- **Arteriosclerosis:** The hardening and loss of elasticity of the arterial walls.
- **Cardiac Hypertrophy:** The enlargement and strengthening of the heart muscle.
- **Stroke Volume (SV):** The volume of blood pumped from the left ventricle per beat.
- **Bradycardia:** A resting heart rate of below 60 beats per minute.
- **HDL/LDL:** High-Density Lipoprotein and Low-Density Lipoprotein.
- **Basal Metabolic Rate (BMR):** The rate of energy expenditure per unit time by endothermic animals at rest.
- **EPOC:** Excess Post-exercise Oxygen Consumption.
- **GLUT-4:** An insulin-regulated glucose transporter found primarily in adipose tissues and striated muscle.
- **Osteoblastic Activity:** The process of new bone formation.
- **Somatic vs. Cognitive Anxiety:** Somatic refers to the physiological symptoms of anxiety (e.g., increased heart rate), while cognitive refers to the mental symptoms (e.g., worry, negative thoughts).
## Practical Skills
### Techniques & Processes
While this is a theoretical topic, it has direct practical application in designing training programmes.
**Designing a Programme to Reduce CHD Risk:**
1. **Mode:** Focus on continuous aerobic exercise (running, cycling, swimming, rowing).
2. **Frequency:** Aim for 3-5 sessions per week.
3. **Intensity:** Work at 60-85% of maximum heart rate (MHR). Use the Karvonen formula for more advanced calculations.
4. **Duration:** Each session should last for at least 20-30 minutes.
5. **Progression:** Gradually increase duration or intensity to ensure progressive overload and continued adaptation.
**Designing a Programme for Weight Management (Obesity):**
1. **Combine Aerobic and Resistance Training:** Use aerobic exercise for calorie expenditure and resistance training to build muscle and increase BMR.
2. **Incorporate High-Intensity Interval Training (HIIT):** HIIT is highly effective at stimulating EPOC.
3. **Monitor Energy Balance:** Educate the client on the importance of a balanced diet in conjunction with the exercise programme.
## Exam Component
### Written Exam Knowledge
This topic is a staple of the written theory paper. Questions will require you to:
- **Identify** the health benefits of exercise (AO1).
- **Explain** the physiological mechanisms behind these benefits (AO2).
- **Analyse** how different types of exercise impact specific conditions (AO3).
- **Evaluate** the role of exercise in public health strategies (AO3).
Expect questions ranging from short 2-mark definitions to extended 8- or 10-mark essays. For longer questions, structure is key. Use an introduction to define hypokinetic disease, dedicated paragraphs for each condition with specific mechanisms, and a concluding summary.
