Study Notes
Overview
This guide covers the core knowledge required for the Sleep Disorders topic within the OCR GCSE Psychology specification. Examiners expect candidates to demonstrate a precise understanding of the differences between Insomnia and Narcolepsy, including their specific symptoms and underlying biological mechanisms. A key focus is the role of the neurotransmitter hypocretin in the context of Narcolepsy. Furthermore, candidates must be able to critically evaluate the effectiveness of treatments, contrasting psychological therapies like CBT-I with drug-based interventions. This requires a firm grasp of AO1 (knowledge), AO2 (application), and AO3 (evaluation) skills. This guide will break down these complex areas, providing clear explanations, worked examples, and memory hooks to ensure the information is retained and can be applied effectively under exam conditions.
Key Disorders
Insomnia
What it is: Insomnia is a persistent difficulty with sleep initiation, duration, consolidation, or quality. For an official diagnosis, these issues must occur at least three nights a week for three months and cause significant daytime impairment. Examiners award marks for distinguishing between the two main types:
- Onset Insomnia: Difficulty falling asleep at the beginning of the night. The physiological mechanism often involves the sympathetic nervous system remaining in a state of hyper-arousal (the 'fight or flight' response), releasing stress hormones like cortisol and adrenaline which are incompatible with sleep.
- Maintenance Insomnia: Difficulty staying asleep, characterized by frequent or prolonged awakenings during the night, or waking too early and being unable to return to sleep.
Specific Knowledge: Candidates must be able to explain the role of physiological arousal and cognitive factors (e.g., negative thoughts about sleep creating a vicious cycle of anxiety) in perpetuating insomnia.
Narcolepsy
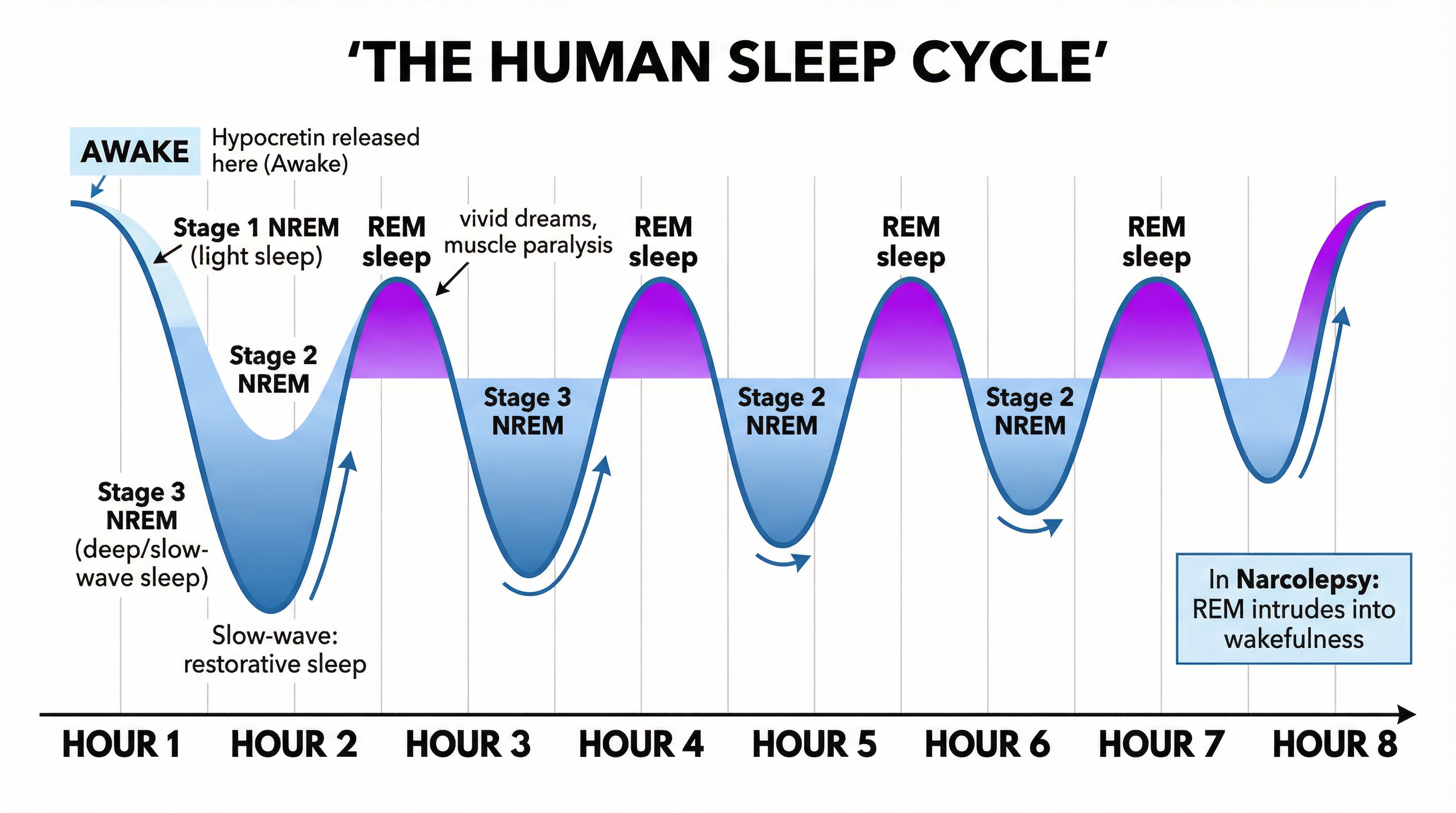
What it is: A chronic neurological condition caused by the brain's inability to regulate sleep-wake cycles normally. It is not simply 'feeling tired'; it involves the intrusion of REM sleep features into wakefulness. This is caused by a profound lack of a key neurotransmitter.
Biological Cause: The primary cause is a deficiency of the neurotransmitter hypocretin (also known as orexin). In most narcolepsy patients, the hypothalamic neurons that produce hypocretin have been destroyed, likely by an autoimmune response where the body's immune system mistakenly attacks its own cells.
Key Symptoms (The Tetrad):
- Excessive Daytime Sleepiness (EDS): Overwhelming sleepiness and sudden, irresistible 'sleep attacks'.
- Cataplexy: A sudden, brief loss of voluntary muscle tone triggered by strong emotions like laughter, surprise, or anger. The person remains conscious. This is a direct manifestation of REM sleep paralysis (atonia) occurring during wakefulness. Crucially, candidates must not confuse this with just feeling weak or tired.
- Sleep Paralysis: A temporary inability to move or speak while falling asleep or waking up.
- Hypnagogic/Hypnopompic Hallucinations: Vivid, often frightening, dream-like experiences that occur at the transition between wakefulness and sleep.
Treatments & Evaluation
Cognitive Behavioural Therapy for Insomnia (CBT-I)
What it is: A multi-component psychological therapy considered the first-line treatment for chronic insomnia.
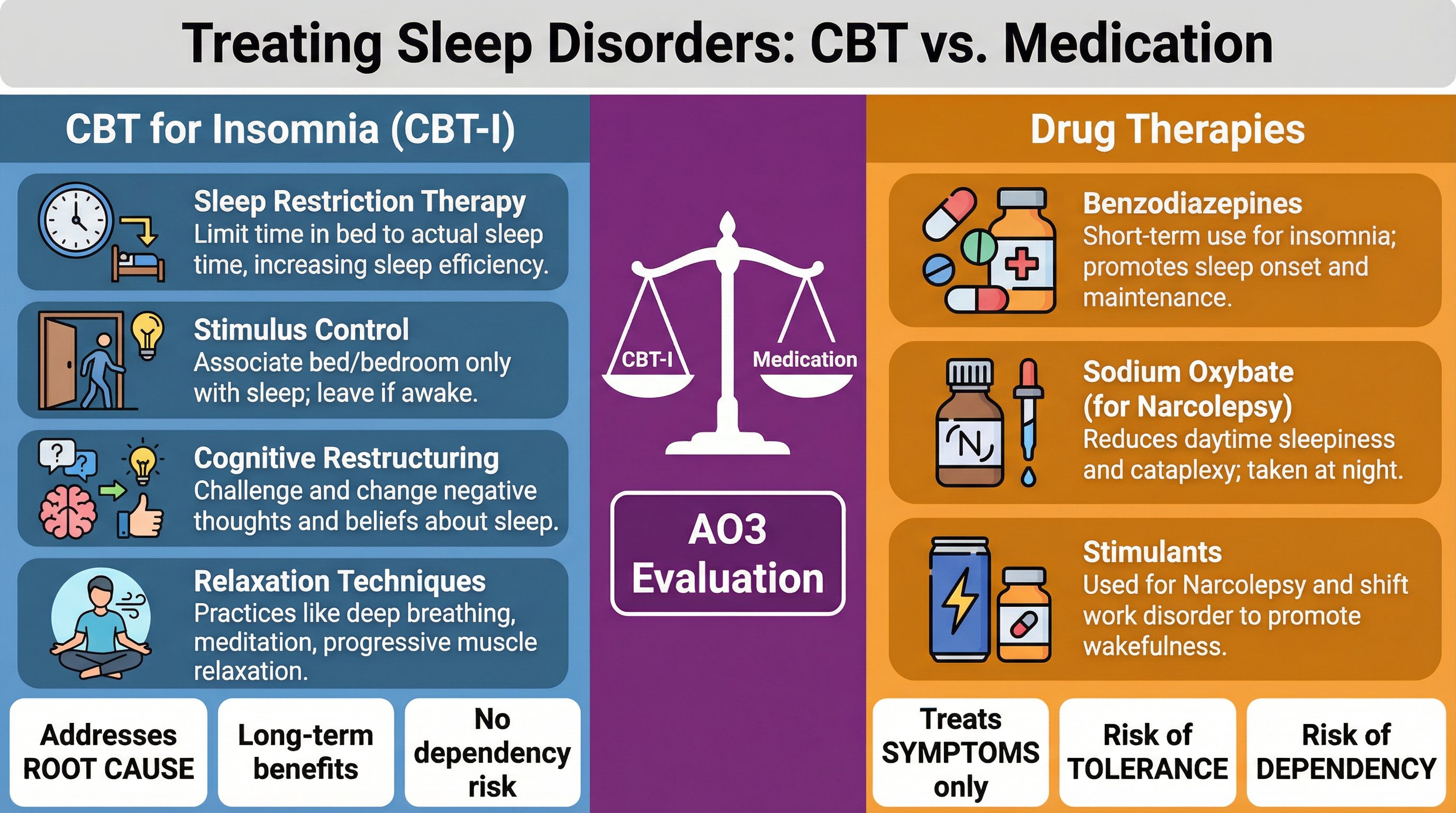
- Key Components: Sleep Restriction, Stimulus Control, Cognitive Restructuring, Relaxation Training.
- Why it matters (AO3): CBT-I is highly effective because it addresses the root causes of insomnia (maladaptive behaviours and cognitive patterns). Its benefits are long-lasting, and it carries no risk of the tolerance or dependency associated with medication.
Drug Therapies
What they are: Medications used to manage symptoms.
- For Insomnia: Benzodiazepines (e.g., Diazepam) enhance the effect of the inhibitory neurotransmitter GABA. They are effective for short-term relief.
- For Narcolepsy: Stimulants (e.g., Modafinil) are used to manage EDS, while Sodium Oxybate is highly effective for consolidating night-time sleep and reducing cataplexy.
- Why it matters (AO3): Drug therapies treat the symptoms, not the underlying cause. For insomnia, they pose significant risks of tolerance (needing more of the drug for the same effect) and dependency (physical or psychological reliance). For narcolepsy, they are essential for managing the condition as the lost hypocretin neurons cannot be restored.
Worked Examples
3 detailed examples with solutions and examiner commentary
Practice Questions
Test your understanding — click to reveal model answers
Outline what is meant by 'onset insomnia'. (2 marks)
Hint: Think about the start of the night.
Explain the role of hypocretin in narcolepsy. (3 marks)
Hint: What does hypocretin normally do, and what happens when it's missing?
A 45-year-old man reports feeling overwhelmingly sleepy during the day, and recently collapsed while laughing with friends, though he didn't lose consciousness. Using your knowledge of psychology, identify and describe the sleep disorder he is likely experiencing. (4 marks)
Hint: The two key symptoms are mentioned in the scenario. Name them and the disorder.
Compare CBT-I and drug therapy as treatments for insomnia. (8 marks)
Hint: Think about effectiveness (short vs long term), what they treat (symptoms vs cause), and side effects (dependency).
Explain how an autoimmune response is thought to cause narcolepsy. (3 marks)
Hint: What is being attacked, and by what?