Psychological Problems — WJEC GCSE Study Guide
Exam Board: WJEC | Level: GCSE
Master the core content for WJEC GCSE Psychology: Psychological Problems. This guide breaks down Schizophrenia and Depression, focusing on the key theories, studies, and evaluation points that examiners award marks for. Secure top grades by understanding how to apply your knowledge with precision.
## Overview
This topic delves into two major psychological problems as defined by the WJEC specification: Schizophrenia and Depression. For candidates, success hinges on precise knowledge of their clinical characteristics, the biological explanation for Schizophrenia (the Dopamine Hypothesis), and the psychological explanation for Depression (Beck's Negative Triad). A significant portion of marks is allocated to applying this knowledge to scenarios and evaluating the associated treatments, namely Antipsychotics and Cognitive Behavioural Therapy (CBT). Furthermore, critical analysis of two specific studies, Daniel et al. (1991) on Schizophrenia and Tandoc et al. (2015) on Depression, is non-negotiable. Examiners expect candidates to move beyond simple descriptions, demanding a clear understanding of the methodologies, findings, and implications of this research. This guide will equip you with the detailed, exam-focused knowledge required to excel.

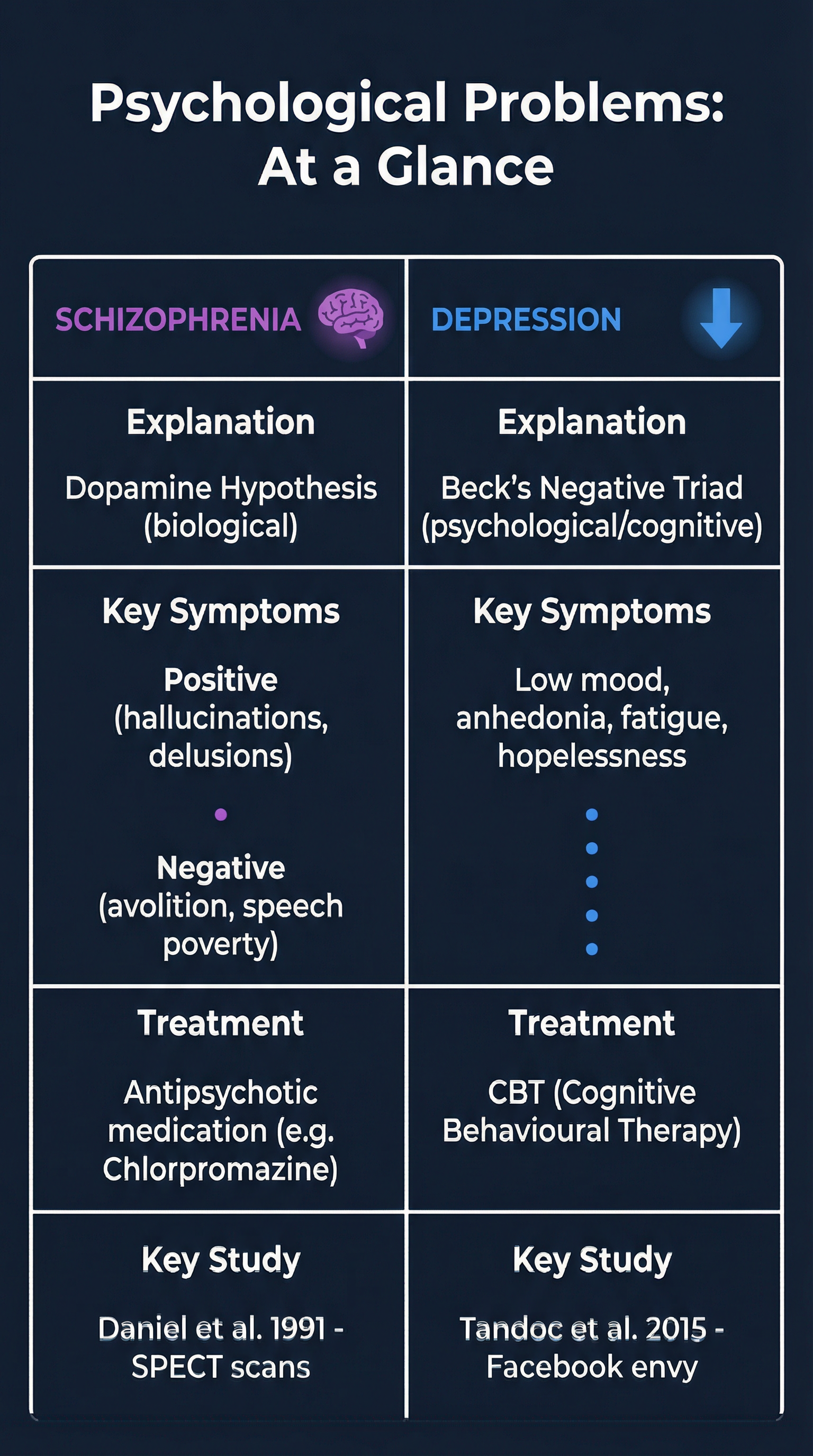
## 1. Schizophrenia
### Clinical Characteristics (AO1)
Schizophrenia is a severe, long-term mental health condition. Its symptoms are categorised by examiners into two types, and confusing them is a common error.
- **Positive Symptoms**: These add an experience that is not present in reality. Credit is given for identifying:
- **Hallucinations**: False sensory experiences, such as hearing voices or seeing things that are not there.
- **Delusions**: False beliefs that are firmly held despite evidence to the contrary, such as delusions of persecution (believing you are being followed) or grandeur (believing you have special powers).
- **Negative Symptoms**: These represent a loss or reduction of normal functioning. Marks are awarded for describing:
- **Avolition**: A severe lack of motivation to complete purposeful activities. This is not laziness; it is a clinical reduction in drive.
- **Speech Poverty (Alogia)**: A reduction in the amount and quality of speech. Responses may be brief and empty.
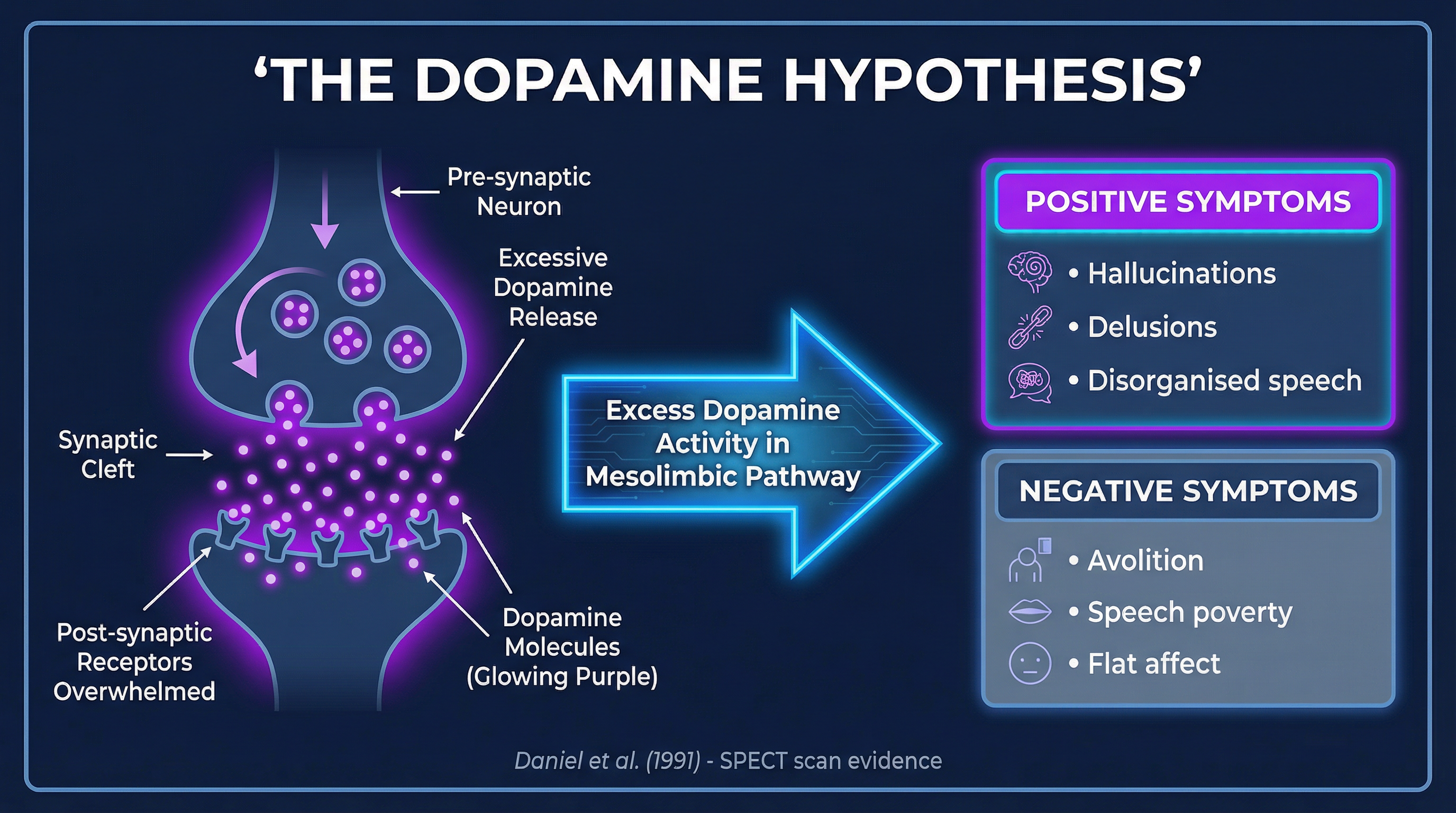
### Biological Explanation: The Dopamine Hypothesis (AO1)
This is the primary biological explanation required by WJEC. It proposes that Schizophrenia, particularly its positive symptoms, is caused by excessive activity of the neurotransmitter dopamine in the brain.
- **Mechanism**: The hypothesis suggests that there are either too many dopamine receptors, or the receptors are oversensitive to dopamine.
- **Brain Areas**: This overactivity is specifically linked to the **mesolimbic pathway**, a key reward and motivation circuit in the brain.
- **Effect**: The excess dopamine activity leads to the acute positive symptoms of hallucinations and delusions.
### Treatment: Antipsychotic Medication (AO1 & AO3)
- **How they work**: Typical antipsychotics (e.g., Chlorpromazine) are dopamine antagonists. They work by blocking D2 dopamine receptors in the synapse, reducing the amount of dopamine that can be absorbed and thus dampening down the activity in the mesolimbic pathway. This reduces positive symptoms.
- **Evaluation (AO3)**:
- **Effectiveness**: Highly effective at reducing positive symptoms, allowing many patients to live functional lives. Atypical antipsychotics (e.g., Clozapine) are also effective for some patients who do not respond to typical drugs.
- **Appropriateness & Side Effects**: Less effective for negative symptoms. Significant side effects are a major issue. Short-term effects include sedation and dry mouth. Long-term use can lead to **tardive dyskinesia**, a condition causing involuntary facial movements. This raises ethical questions about patient consent, especially when a patient lacks insight during a psychotic episode. The high likelihood of side effects leads to issues with patient compliance (stopping medication).
### Key Study: Daniel et al. (1991)
- **Aim**: To provide evidence for the Dopamine Hypothesis using modern neuroimaging.
- **Method**: Used **SPECT scans** (Single Photon Emission Computed Tomography) to study brain activity in patients with Schizophrenia. Participants were given an injection of **amphetamine**, a drug known to increase dopamine levels.
- **Findings**: The amphetamine administration was correlated with an increase in psychotic symptoms. The SPECT scans confirmed that this was linked to increased dopamine activity in the brain.
- **Conclusion**: This provided direct, scientific evidence supporting the link between dopamine function and the symptoms of Schizophrenia. For the exam, you MUST name the scanning technique (SPECT) and the drug (amphetamine) to gain full credit.
## 2. Depression
### Clinical Characteristics (AO1)
Depression is a mood disorder characterised by a persistent feeling of sadness and a loss of interest. Key characteristics include:
- **Low Mood**: An enduring and pervasive feeling of sadness.
- **Anhedonia**: A loss of interest or pleasure in activities that were once enjoyed.
- **Fatigue**: Significant loss of energy.
- **Cognitive Symptoms**: Feelings of worthlessness, guilt, and hopelessness; difficulty concentrating.
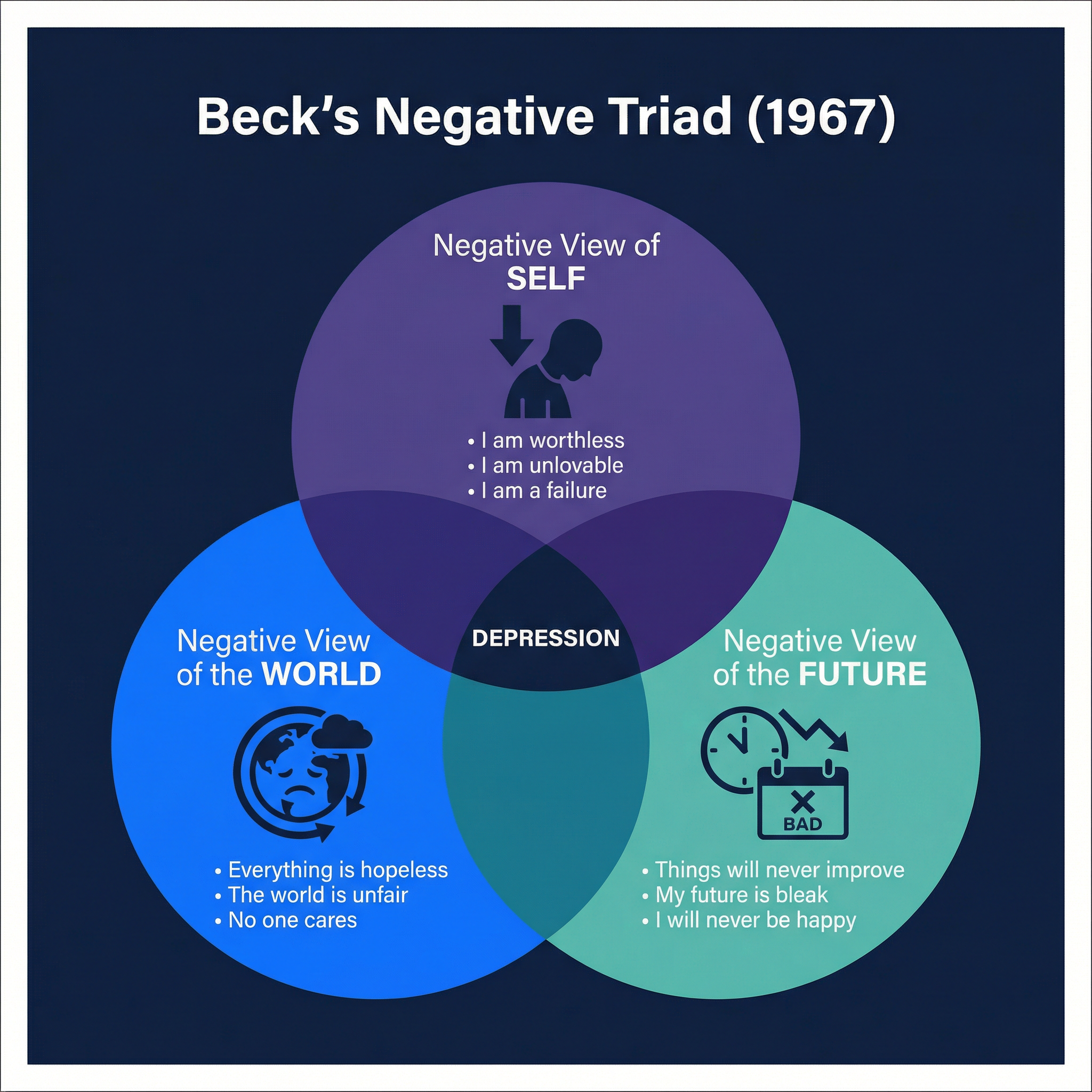
### Psychological Explanation: Beck's Negative Triad (1967) (AO1)
Aaron Beck proposed a cognitive explanation for depression, suggesting it stems from a person's faulty and negative thinking patterns.
- **The Triad**: This consists of three interconnected negative thought patterns (schemas):
1. **The Self**: A negative view of oneself (e.g., "I am worthless, I am a failure").
2. **The World**: A negative view of the world (e.g., "The world is a cruel place, nothing ever goes right").
3. **The Future**: A negative view of the future (e.g., "Things will never get better, my future is hopeless").
- **Mechanism**: Beck argued that these negative schemas are activated by stressful life events and lead to a cycle of automatic negative thoughts, which in turn cause the emotional, behavioural, and physical symptoms of depression.
### Treatment: Cognitive Behavioural Therapy (CBT) (AO1 & AO3)
- **How it works**: CBT is a talking therapy that aims to identify, challenge, and change the irrational negative thoughts identified in Beck's model. A therapist helps the client to:
1. **Identify** automatic negative thoughts.
2. **Challenge** these thoughts by looking for evidence that contradicts them.
3. **Replace** the distorted thoughts with more balanced, rational ones.
- **Evaluation (AO3)**:
- **Effectiveness**: Very effective for mild to moderate depression. Research (e.g., Butler et al.'s meta-analysis) shows it has a large and lasting effect. It equips patients with lifelong skills to manage their mental health.
- **Appropriateness**: It is highly appropriate as it has no side effects and empowers the patient. However, it requires significant motivation and commitment from the patient, which can be very difficult when experiencing avolition or fatigue. It is also costly and can have long waiting lists on the NHS.
### Key Study: Tandoc et al. (2015)
- **Aim**: To investigate the link between Facebook usage and depression.
- **Method**: A survey-based correlational study. They measured participants' Facebook use, specifically focusing on **Facebook surveillance** (passively looking at others' profiles and posts without interacting).
- **Findings**: They found a significant positive correlation between the amount of Facebook surveillance and feelings of **envy**. This envy, in turn, was a significant predictor of depressive symptoms.
- **Conclusion**: The study suggests that the social comparison that occurs during passive Facebook use can lead to envy, which is a pathway to depression. Candidates must report this specific chain: **Facebook Surveillance → Envy → Depression**.